Recently, I was able to witness the refugee camp conditions myself. In July 2017, I traveled to Amman, Jordan, where I volunteered at three refugee camps. Speaking to the refugees and listening to their stories was heartbreaking. Many did not have access to food, water, or medicine unless given to them by various organizations. I also met a few people who were physically disabled due to the conflict; they explained how the current condition of their camp did not help them at all. Many had to escape Syria by foot or crammed in the back of a truck. This is neither safe nor accessible to many disabled persons. Many individuals did not have access to essential resources that we use daily, especially disability-accessible resources. The effects of COVID-19 have only worsened the situation. Since the pandemic began, the UN refugee agency has reported that eighty-four percent of refugees with disabilities cited food insecurity as their biggest concern in Lebanon.
“Too often invisible, too often forgotten, too often overlooked,” is how Light for the World describes refugees with disabilities. With the population of refugees increasing, the concern for their protection and access to resources is left unknown. Refugees and displaced persons are individuals fleeing from war-torn countries, poverty, and hunger. They are often neglected and not provided with the proper care and resources, especially those with disabilities. Many have had disabilities on their way to escaping or were born with some form of disability. In the aftermath of the Syrian war and current conditions in Afghanistan and Haiti, many individuals attempt to flee to find protection and asylum. It’s essential to recognize that many displaced individuals, especially those with disabilities, cannot access the necessities they need to live adequately.
Disabilities within the Displaced Communities
Article one of the Convention of the Rights of Persons with Disabilities (CRPD) classifies that “persons with disabilities include those who have long-term physical, mental, intellectual, or sensory impairments, which in interaction with various barriers may hinder their full and effective participation in society.” It’s been noted that more than sixty percent of Syrian refugee households contain at least one person with a disability. Additionally, it has also been reported that twenty-eight percent of persons with disabilities list illnesses or diseases as the primary cause of their disability. These illnesses are brought by the vulnerable conditions they are living in. Although there have been reports of disabilities from birth, most statements have been stated to have disabilities caused by conflict.
Source: Yahoo Images
Individuals with disabilities are already a vulnerable group of people, and refugees with disabilities have even less access. Disabled women are the most vulnerable as they experience “psychological, sexual or physical abuse in natural disasters and conflicts.” Organizations such as the Human Rights Watch (HRW) have urged world leaders providing aid to take more action in funding at-risk groups, such as individuals with disabilities. Emina Cerimmovic, a senior disability rights researcher at HRW, stated that even with all the commitments to better reach persons with disabilities, “displaced people with disabilities continue to struggle even to get basic services.” An international call for action is needed to ensure displaced persons with disabilities can access the necessities required to survive.
Conditions of Refugees with Disabilities
It comes as no surprise when learning how fragile and inaccessible conditions in refugee camps are. Most of these camps are created by the displaced persons themselves. World leaders and governments have shown commitment to protecting refugees and displaced people by providing aid, asylum, and new areas to live. However, these support systems do not take the needs of people with disabilities into account.
Source: Yahoo Images
What’s Next?
Assessing the conditions many refugees with disabilities live in and ensuring that their needs are met is imperative. As the situation grows more dire, what can the world do to better the conditions and resources for refugees and displaced persons with disabilities? The main problem is the lack of and slowness of implementation of aid from world leaders. The information of what is needed has been provided to countries around the world and NGOs, but resources are yet to be delivered. The international community needs to provide aid specifically for those with disabilities, accessible camps need to be built, and medical attention needs to be supplied more. NGOs currently operate only under donations, so provisions are limited by a lack of funding.
What Can You Do?
As we have access to many daily necessities such as food, water, disability-accessible bathrooms, and resources, many worldwide do not. It is essential to learn and educate ourselves about the current situations that hinder many lives. Check the resources below to donate or learn about organizations providing aid to refugees and displaced persons with disabilities.
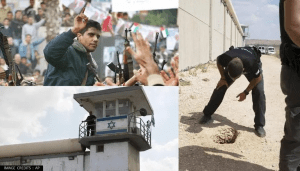
On September 6th, 2021, six Palestinian prisoners escaped from what is known as Israel’s most secure and guarded prison, Gilboa Prison. An escape conducted only with a spoon has been heralded as a heroic victory for the Palestinian people and a major security breach to the Israeli government. The conflict between Israel and Palestine is nothing new. In fact, it’s known by many as a “100-year-old issue.” Since 1948, there have been continuous arguments and battles about land control, but it has now come to be much more. Today, Israel occupies most of the West Bank and has built settlements that are illegal under international law. Aside from speaking about which country controls what land, it is vital to recognize and understand the countless human rights violations happening—most of which were committed by Israel.
Yahoo Images
Israeli Prisons
Since 1967 over one million Palestinian people and supports have been arrested in Israel by the IDF. In June 2021 alone, a total of4650 political prisoners were detained. 200 which were children, 40 women, and 544 serving life sentences. In 2020, there were 700 sick patients arrested and not receiving theproper care. It’s been noted that the Israeli police have targeted Palestinians with discriminatory arrests, torture, and unlawful force. The main targets of arrest are typically Palestinian activists, like the six prisoners who escaped.
In Israeli prisons, Palestinian prisoners live in “appalling conditions that are subjected to harsh treatment.” The United Nations hasnoted that techniques used by the Israeli General Security Service during prison interrogations constitute torture. Once arrested, prisoners and detainees begin to endure physical abuse and humiliation—allviolations of international humanitarian and human rights law. When interrogated, they become exposed to “physical torture and psychological intimidation.” They are beaten, put into solitary confinement, inspected, deprived of medical and sanitary resources, and many more things. The report confirmed these conditions and the treatment of Palestinian prisoners in Israeli prisons through multiple letters sent to the UN and posted.
In addition to the illegal conditions of arrests and detention, Palestinian children have become increasingly targeted by Israeli detention. These children have been abducted and denied their fundamental human rights, sentenced, and convicted throughout the night. About 95% of the Palestinian children released from Israeli jails suffer from torture and ill-treatment during their time spent and throughout the interrogation process. Sick detainees have also been a massive problem within these prisons. More than 1,500 Palestinian prisoners—including those with disabilities—suffer from different physical and mental illnesses due to the poor conditions and no access to medical attention. Prisoners with cancer are denied any type of access to medical attention unless it is an emergency. Meaning chemotherapy is not an option. Routine doctor’s visits, medicine, anything a typical cancer prisoner should be provided, is not allowed. The condition of these prisons continues to worsen and violate human rights.
The Re-Capturing of the Six Prisoners
The news of six prisoners escaping comes as a surprise to everyone. Not one person, Israeli or Palestinian, would have imagined that not one but six people could ever escape again. Once the world knew six people had escaped, the Israeli government began a search to find all six of them. The escape set off anuproar within the Israeli government as it was the biggest jailbreak seen in more than twenty years. Since the escape, Israeli prisoners have doubled down on their security, causing many Palestinian prisoners to protest and go on hunger strikes. With the current prison situation, it’s not imaginable what constitutes stronger security conditions. This is known as “collective punishment”, which is deemed illegal under humanitarian law. Posts around social media show the different forms of protests the prisoners have been doing. In addition, the manhunt included harassment of family members and violent raids across the occupied West Bank and East Jerusalem. The recapturing of the prisoners resulted in protests in the occupied West Bank and around the world.Thousands gathered to protest the rearrest and the reasons for the original arrests. Protesters in Palestine went out “in solidarity without prisoners in the occupier’s jails… it’s the least we can do for our heroic prisoners,” saidJihad Abu Adi.
Yahoo Images
Since being captured, the escapees have all been tortured and beaten by the Israeli occupation forces. The worst being towards Zakaria Zubaidi. After he was rearrested, he was tortured so badly; he had to be sent to the ICU to receive urgentmedical treatment. He was taken toRambam Medical Center, located in Haifa, for treatment. It has been suspected that Zubeidi was tortured with electricity. His brother released a statementsaying, “my brother is being subjected to the harshest form of torture.” Along with the electric form of punishment, it is noted that Zubeida’s leg was broken, and the Israeli prison forces did not allow him to sleep. Israeli security forces also did not allow lawyer visits for any of the recaptured. Palestinian human rights groups have asked the International Red Cross to get involved and facilitate interactions between their legal counsel and their families.
What’s Next?
Many Palestinians continue to live in fear of what is to come after the prison break. In the midst of fear, victory is sensed. Many journalists, Palestinians, and supporters have called this a momentous victory that showcases the strength and resilience of countless Palestinians.
Yahoo Images
The most important thing one can do is learn the history, educate themselves, and read. Many individuals are being treated in an unfair manner which is deemed illegal under International Law.
Check out these links, social media accounts, and books to learn more. @eye.on.palestine, an account on Instagram, posts daily updates on the occupation forces attacking Palestinians. Additionally, their accounts share pictures and post stories of what it’s like to live in an Israeli prison, access to medical care, and the food strikes conducted in protest.
Books:
My Promised Land: The Triumph and Tragedy of Israel, Ari Shavit
In Search of Fatima: A Palestinian Story, Ghada Karmi
Arabs and Israelis: Conflict and Peacemaking in the Middle East, Abdel Monem Said Aly, Shai Feldman, Khalil Shikaki
The Texas Abortion Law, signed into law on May 19th, 2021, went into effect earlier this September, effectively banning abortions after the detection of fetal heartbeat. This law makes no exceptions even for victims of rape or incest.
Previous abortion bills introduced the state government and authorities to enforce abortion laws, but unlike anything seen before, Texas’s law awards the power to the citizens. Any private citizen in the country now has every right to sue anyone they suspect has had an abortion, took part in helping with an abortion, or in any way assisted an individual seeking an abortion in Texas. If the suit succeeds, the citizen will receive monetary compensation of at least $10,000. The intricacies of this law make it difficult to legally interpret since technically, abortion has not been criminalized.
History of the Heartbeat Bill
In 1973, the landmark Supreme Court case Roe vs. Wade federally legalized abortion in the first two trimesters of pregnancy but allowed states toban abortion in the 3rd trimester. Since then, several state legislatures have passed so-called “heartbeat bills,” which criminalize abortions after fetal cardiac activity has been detected—usually at 6 weeks. However, this is only a flutter of electricity, and the heart forms only after 17-18 weeks. Most individuals do not even know that they are pregnant at this point, because birth control, other forms of contraception, or not tracking menstrual cycles can mask pregnancies until the 8th week.
Up until now, the Supreme Court has adamantly upheld Roe vs Wade, and every state abortion ban signed into law has been struck down in federal courts.In a historic decision, the United States Supreme Court ruled to let Texas temporarily implement its Abortion Law Although the decision was made in consideration of the difficulty interpreting the law by the Constitution, the hesitancy has been raising alarms all over the country.
Despite the common misconception that abortion restrictions reduce abortions, they only increase unsafe abortions. Women and young girls use dangerous methods such as toxic chemicals, bodily harm, and relying on unlicensed abortion providers in their desperation to terminate a pregnancy. In fact, in the United States, the American College of Obstetricians and Gynecologists (ACOG) found that over 1.2 million women had unsafe abortions which resulted in nearly 5000 deaths, not including tens of thousands more left with long-term injuries and complications.
Source Unsplash: Protestor holding up a placard stating “Protect Roe” in an October 2021 protest against Anti- Abortion Laws.
Women in Texas Now
The state has clearly indicated that the law is “not against women” but against abortion providers who are breaking the law.
Already, women in Texas are traveling out to liberal states such as California or New York to get their abortions. The influx of cases has overburdened providers in other states, but even still, those who make it out of state to receive an abortion at least have the option. The majority of women, however, do not have the means or funds to obtain an abortion in another state, so they turn to abortion pills to self-induce abortions. This method has its own problems. The pills can get stuck in customs anywhere from 2 to 30 days which adds to the anxiety of pregnant individuals, because the pills must be taken before 10 weeks of gestation to avoid life-threatening complications such as massive hemorrhaging.
Political Reaction
The Texas Abortion Ban symbolizes the modern bodily autonomy movement on a precipice. Based on the Supreme Court’s current balance, it is possible that Roe vs. Wade could be struck down within the next two years. One thing must be made clear though: overturning Roe vs. Wade means that abortion will only become illegal within states that have chosen to do so—not across the country.
However, another aspect to consider about the abortion rights debate is voice. Women and minorities are more empowered than four decades earlier and have the platform to fight for their beliefs. In fact, 77% of people want the Supreme Court to uphold Roe vs. Wade. If Roe vs. Wade is overturned, an unprecedented amount of public outcry will occur in every state to fight, once again, for the right to bodily autonomy that women have fought for decades.
Source: Unsplash; An Abortion Rights billboard titled “Forward Together for Abortion Justice” at a protest in October 2021.
Future
Later this year, the Federal Courts will hear Mississippi’s case to let their heartbeat law stand for 15 weeks. More conservative states will likely use Texas’s law to support their legislations. Thus, the outcome of these hearings will give the country an understanding of how the federal judicial system will respond to future abortion and women’s health legislation.
In the Senate and House of Representatives sits a bill titled the Women’s Health Protection Act, which could provide universal abortion rights and remove the damaging restrictions women are subjected to for abortions. One of the goals of women’s rights activists is to see this bill passed in Congress, and the time has come for Congress and the Executive Branch to collaborate and alleviate any detrimental decision that the judicial system may make. The public can help with this goal by proactively voting for legislators that will turn bills into reality and supporting many nonprofit organizations and charities such as NARAL Pro-Choice American and Planned Parenthood through volunteer work or donations.
Bhutan is often referred to as an idyllic Himalayan nation, a land of peace and prosperity, happiness, and beauty. After visiting Bhutan in 2017, I was even more fascinated, and truly began to understand why the small, neutral country has been dubbed a “real-life Shangri-La”. It is the only nation in the world to measure annual success by Gross National Happiness, rather than Gross Domestic Product. It is also the only country to have a carbon-negative footprint, with extraordinary levels of hydropower and renewable energy production and a zero-tolerance policy for industrial development. Bhutan is rapidly decreasing poverty rates and increasing the middle-class population. Government programs have made education and trade school accessible to most citizens who desire it. Bhutan has managed to remain neutral for hundreds of years with a minimal military presence despite being nestled between two conflicting superpowers, India and China. Citizens of Bhutan enjoy the state’s extensive social welfare programs and are enamored with the royal family that abdicated power to allow a peaceful transition to a democratic system.
In short, the nation seems like a true paradise, where culture and tradition are preserved with love and care, where nature is respected and upheld, and where one can pursue life to the fullest in a land of prosperity and opportunity. When I had the opportunity to travel through Bhutan, I was stunned by the gorgeous landscape, nation, and culture. I was welcomed with clearer air than I thought possible, a colorful landscape filled with trees and prayer flags, and adorable buildings constructed in traditional Bhutanese fashion. The people were so happy, and talked passionately about their country, royal family, and culture. There is a strong sense of nationalistic pride, and from everything Bhutan boasts, it seemed to be entirely deserved. Our guide taught us about local customs, Bhutanese Buddhism, traditional dress and building style, and masterfully escorted us through the most beautiful aspects of Bhutan and its culture.
It was only after leaving that I learned of human rights abuses Bhutan so carefully hides from tourists. Our state-sanctioned tour guide was an instrument in how this flawless reputation has been skillfully crafted, and the execution was so perfect that nothing felt staged while I was there. I enjoyed the country within an intricate veil of ignorance, unaware of the atrocities that no one is allowed to see.
Bhutanese children. Source: World Bank Photo Collection
Violations Exposed
Bhutan may appear to be a nation without error, but the country has perpetrated major human rights violations since the 1980s. For four decades, the United Nations, Freedom House and Human Rights Watch have consistently criticized and exposed Bhutan’s human rights violations. The nation is limited by strict libel laws and a culture that is unwilling to speak negatively on the king or his policies. While free speech is protected under Bhutan’s constitution, it is rarely practiced and this self-censorship is coupled with a flawed judicial system that harshly punishes those found to be committing the dangerously broad charge of libel. In 2016, a Bhutanese reporter faced libel fines of up to 10 years salary for critiquing a prominent businessman on Facebook. With penalties like this, it is no wonder that citizens of Bhutan do not dare criticize the crown, even though free speech is allegedly protected. Bhutan has been on a Human Rights Watch list since the 80s due to prolific persecution of ethnic minorities. While Bhutan has received credit for its positive changes since transitioning into a democracy in 2008, they still have a long way to go before they can be considered a free nation.
Bhutanese refugees. Source: Creative Commons
Ethnic Cleansing Pre-Democracy
The horrific treatment of the Lhotshampa people in Bhutan is the most atrocious human rights violation known to be committed by the Bhutanese government. The Lhotshampa people are Bhutanese residents with Nepali ethnic backgrounds, who have lived in Bhutan for generations but still speak a separate dialect and have a differing culture from the majority in Bhutan. In order to understand the current plight of Nepali migrants in Bhutan, we must understand a little bit of the once-neighboring nation, Sikkim. Sikkim was once an established monarchical state with most of its population being of Mongolian/Tibetan descent as Sikkimese, just like the ethnic Bhutanese. However, Sikkim faced a mass migration of ethnic Nepalis (of Hindu and Indo-Aryan descent) that caused the people of Sikkim to become a minority in their own nation. Sikkim fell as an independent state and was annexed by India in the 1950s, and the leaders of Bhutan have used the fall of Sikkim as a fear-inspiring example ever since. It is this nationalism and fear of losing sovereignty to one of the superpower neighbor states that has created such a widely supported systemic oppression of the Lhotshampa people in Bhutan.
Bhutan faced its greatest human rights violations in the 1990s, as strong nationalism and resentment towards the Lhotshampa people came to a boiling point. The refugees crossed the border with tales of an ethnic cleansing occurring in Bhutan, stating they were given mere days to sell their homes and were marched from rural villages to Nepali refugee camps. The government’s forces accompanied the refugees across the border with loaded guns and photographers, and according to a Lhotshampa teen interviewed by the Human Rights Watch, “[They] told me to smile…He wanted to show that I was leaving my country willingly, happily, that I was not forced to leave”. It is estimated that the total number of refugees produced in the 1990s was just above 100,000, which is absolutely astounding when we look at Bhutan’s current national population of 780,000. While Bhutan is often portrayed as a modern “Shangri-La”, the seemingly idyllic Himalayan country created more refugees per capita than any other nation in the world in our recent history. Of those 100,000 refugees, 85% have now been rehoused in the United States.
Bhutanese man with child. Source: Creative Commons
Democratic Safeguards Fail
Despite the nation peacefully transitioning towards a democratic state in 2008, the new government has continued the systematic harassment of the minority group, even increasing certain anti-Lhotshampa policies. While the Lhotshampa are no longer persecuted as openly as they were in the early 1990s, they still face significant discrimination within the nation their families have called home for generations. Out of countless treaties currently in existence to protect and defend human rights, Bhutan has only signed two. Bhutan signed the Convention on the Rights of the Child (CRC) in 1990, and many within the international community argue that Bhutan has violated the convention due to the large population of children within the persecuted Lhotshampa refugees.
Perhaps the most recent evidence proving such discrimination came with Bhutan’s new constitution in 2008, when Lhotshampa people discovered their citizenship was up for debate, and access to passports and documentation became determined by financial, marriage, or literacy status, which is very reminiscent of the second-class citizenship African Americans faced in the United States. Some of the limitations imposed upon Lhotshampas with these targeted passport systems are the inability to travel internationally, which is a blatant violation of both the right to Freedom from Discrimination and the Right to Movement established in the Universal Declaration of Human Rights. One of the brilliantly cruel aspect of the passport stipulations is that while Lhotshampa people may freely leave the country, it is extremely unlikely that they will be allowed to return. For many, a trip to visit neighboring India or Nepal is the termination of calling Bhutan their home. Essentially, the Bhutanese government made it abundantly clear that Lhotshampas are not welcome in Bhutan.
In addition, while there is no clear law preventing Lhotshampas from purchasing property or moving freely within Bhutan itself, it is extremely unlikely in practice that Lhotshampas will be able to secure property or livelihoods outside of specific regions that have become socially designated for them. Bordering nations like Nepal continue to host new refugees fleeing a land many consider to be peaceful, sacred, and free of worldly troubles. Lhotshampas have continued to cross the Nepali border to refugee camps since 2008 purely out of desperation from lack of work or freedoms in Bhutan. Websites like these provide some much needed insight into the current plight of the Lhotshampas, as well as what life is like for those still awaiting rehousing inside of their temporary refugee camps.
Refugees outside of a hut. Source: United Nations
How to Help
In order for change to be made, Bhutan needs continual pushes from the outside world. By spreading the true story of the Lhotshampa people and looking for ways to get involved, you are directly contributing to decades old efforts to ease the horrors they face. Creating action on any level is an excellent way to assist the Lhotshampa people and refugees like them. If you would like to donate or volunteer to assist Lhotshampa refugees, there are countless local and international efforts that will put anything you can give to great use. Reputable non-profits like Sewa USA use funds to provide necessities, transportation and employment help for Bhutanese refugees in the United States, and the World Food Programme uses donations to provide food and resources to Lhotshampas still displaced in refugee camps. Ultimately, resource-based aid is an excellent way to assist those who have been cruelly displaced and discriminated against, but only international pressure for domestic changes within Bhutan will be able to stop the persecution and prevent any more Lhotshampas from becoming refugees.
Source: Yahoo Images; People experiencing homelessness sleeping under a bridge
The homeless population in America tends to be neglected by the society they live in. They are among the most vulnerable, belonging to already marginalized communities that struggle to meet their day to day needs. As a result, the unhoused have little to no power or influence on social norms and affairs. As someone who has experienced homelessness both in India and in America, I have come to distinguish some of the common misconceptions society holds about the unhoused population. There are a lot of stereotypes and social stigma that surrounds the discussions around homelessness, which often blames the victims of systemic issues, instead of restructuring the conversation around how we as society can best help these marginalized groups realize their basic human rights to shelter. In order to do so, we must first understand what it really means to be homeless in America.
History of Homelessness in America
Homelessness is not an issue unique to the United States, as it can be found in countries all over the world. While homelessness in America can be found as early as the colonial times, modern homelessness rose as a response to the Great Depression, where people experienced high levels of unemployment and poverty. Especially interesting is the relationship between the growth of urban cities and the rise in homelessness. Coupled with low-wages and higher costs of living, people found it more expensive to find places to live in urban centers, such as New York and California. The aftermath of the Great Depression put a lot of people in desperate need of employment, and as the economy took to the service industry, more and more undereducated, impoverished people had no other choice but to turn to these low-income jobs. The country’s shift to a service economy meant that laborers were now being paid lower wages, leaving service industry employees unable to afford the rising costs of housing. Coupled with higher housing costs and lower wages, when people turned to social welfare programs, they found these programs to be lacking in funds as well.
Additionally, there was a campaign to “Deinstitutionalize” people held in mental asylums. While the campaign itself was well-intended, its applications were lacking in structure, and instead of providing patients with proper access to mental health resources, people with mental disabilities were released to fend for themselves. The neglect of these institutions led to the increasing numbers of mental health patients facing housing insecurity. To make matters worse, gentrification policies (made to bring in wealthy real-estate investors and high-income residents to underdeveloped parts of the city) led to the displacement of many low-income families, putting them out of their homes. These policies disproportionately affect people of color, something that has forced many marginalized communities to fall prey to an endless cycle of poverty and degradation.
Unfortunately, one of the most concerning additions to the homeless population is the disproportionate number of youths that identify as being part of the LGBTQ+ community. According to a recent study conducted by Chapin Hall at the University of Chicago, LGBTQ+ youth had a 120% higher risk of experiencing homelessness. These members who already belong to an ostracized community can become more vulnerable to harassment, violence and hate crimes.
Additionally, unable to find jobs after returning home from military service, many veterans end up homeless with nowhere else to go. Although places do exist to support veterans who experience homelessness, many are either unaware of the resources at hand, or too ashamed to use these resources. As a result of the social stigma surrounding the topic, people experiencing homelessness often become withdrawn from society.
Society’s Attitudes Toward the Homeless
Source: Yahoo Images; An example of hostile architecture that prevents the unhoused from sleeping on benches
Homelessness is received with wildly different attitudes among different cultures. America is a very diverse country, with people that share hundreds of different cultures and traditions, and these cultural attitudes can carry over in the way they respond to contemporary social issues. Different cultures share a varying definition of what a “home” means, and even more distinctions in their approach toward people experiencing homelessness. What the dominant White culture might consider to be a home, (an individual unit of space for nuclear families), might not be what someone who belongs to the Indigenous population believes. They might argue that a home is where you can interact with your community, a place to feel safe and share with friends and family. Even the attitudes toward helping people who are unhoused have strict cultural implications. As described in Islam, it is part of the every-day religious ritual of a Muslim to give alms and help the poor in their community. In Hinduism, while helping the poor with food and shelter is allowed, certain castes are not allowed to eat alongside with or sit beside people of lower castes. People experiencing homelessness have their own unique culture, where certain skills or strategies for survival on the streets are shared amongst each other.
Along with all these complexities, the unhoused also undergo various types of stigmas, including social stigma, and cultural stigma. Social stigma can be discrimination and harassment directed toward the homeless population by the institutions, systems and people that make up society. Cultural stigma can refer to the stigma expressed by friends and family members or other religious or cultural institutions that may shame and blame the victims for being homeless.
Unhoused people also have a hard time finding employment. This is partly due to the fact that the job application requires a home address for the application process to be completed. As a result, people who are dispossessed also experience difficulties when finding housing. The applications for apartments include a proof of income/employment section and applying for government housing takes months to be processed and reviewed. Many states have long and complicated application processes, and even then, it is not a guaranteed housing option. Nevertheless, applicants can be denied, and they would still need a place to stay while awaiting their application to be approved.
Adding to these difficulties, people in the homeless community are constantly harassed with wild stares or abuse, (both verbal and physical), from members of society. The law enforcement agency, an institution designed to serve and protect people of the community, may make matters worse by deteriorating the situation further. Without proper training, police approach the homeless defensively, ready to attack at the slightest “abnormal” reactions. What they haven’t been trained to realize is that many people experiencing homelessness are also at high-risk of developing mental health issues due to the stress and realities of being homeless. These altercations can turn deadly, and unfortunately, many people of the homeless community have either been locked up or even killed by officers of the law. Many of these instances were even caught on camera, yet these officers faced little to no accountability or legal punishment.
People experiencing homelessness are also easy targets to getting their possessions robbed, and many times, police will raid their camps and confiscate what few belongings they might acquire, including sleeping tents and toiletries. Society also treats the homeless population as a burden and blames them for being “lazy” or “druggies” or “criminals/suspicious,” without any provocation from the homeless community. It can be especially insulting for the people experiencing homelessness to be judged for their situation while society simultaneously fails to criticize the state’s inability to protect peoples’ fundamental human rights to food, shelter, and other basic needs.
The Legal Response to Homelessness in America
Source: Yahoo Images; An example of hostile architecture to deter the homeless from sleeping under bridges
The legal response to the homelessness crisis in America has not been a heartwarming one either. Urban cities all over the United States have put in place anti-homelessness measures, otherwise known as hostile architecture. These include slanted benches, benches divided by armrests, spiked and rocky pavements to prevent people from sleeping there, and even boulders under bridges. Not only are these measures inhumane, they also cost the tax-payers a lot of money. These atrocious tactics are put in place to discourage homelessness, attempting to connect rising numbers of homelessness to increased crime rates. As recently as July of this year, Los Angeles even went so far as to make homelessness downright illegal, restricting homeless encampments in majority of the city. The city has even prohibited the homeless from sitting, sleeping, or laying in public. Due to the fact that homelessness overwhelmingly affects people who belong to already marginalized communities, a rights-based approach is necessary, one that addresses the existing systemic issues which need to be fixed first.
Covid-19 and How it Continues to Impact the Homeless Population
Source: Yahoo Images; Homeless shelters can be crowded, without proper social distancing measures in place
The Covid-19 pandemic continues to impact many different communities in a variety of ways. The pandemic hit especially hard among the homeless population, where access to hygienic products are often slim, if not non-existent. People experiencing homelessness may not have the ability to continuously wash and sanitize their hands, with limited access to clean water and soap products. They also been experience complications with social distancing measures, forced to be in crowded spaces like homeless shelters, which has only increased their risks of getting infected. Furthermore, even when infected, or exposed to the disease, the homeless population has very limited ability to quarantine, further allowing the spread of the disease to others in close proximity. The unhoused population has limited access to healthcare and medicinal treatments, and many are already immunocompromised or have pre-existing conditions, which increases their vulnerability of catching the disease. Stereotypes geared toward the homeless population labeling them as “junkies” or “druggies” has influenced the care they receive, leading to many cases of misdiagnoses or mistreatment as a result of biases held by healthcare professionals and others in the health care industry. Due to the rise in unemployment numbers during the economic shutdown as a response to the pandemic, millions of people who did not qualify for unemployment benefits, and could not make ends meet, also became homeless as a result.
Some Successful Approaches to Ending Homelessness
source: yahoo images; An unhoused person advocating against hostile architecture
There have been some successful attempts at ending homelessness in America as well as in other nations. Utah attempted to decrease its rates of homelessness back in 2015, which successfully reduced its homelessness by 91%. They executed a policy known as “Housing First,” which gave their chronically homeless populations free housing, a decision that cost the state less money than alternative anti-homelessness measures. This program unfortunately has not been a complete success, as people experiencing homelessness in other states have been migrating to Utah, making it too expensive for Utah alone to pay for the country’s increasing homelessness crisis. A national policy, on the other hand, that could implement the Housing First approach taken by Utah, may be the easiest, and essentially cheapest option to ending the homelessness crisis in America. This is essentially what Finland did. In 2019, Finland approached the homelessness issue with the most obvious of answers, by providing housing for all those who are unhoused. Like Utah, they applied the “Housing First” policy, (which came with no strings attached), recognizing that housing is an essential human right that should be protected and promoted. They also understand that in the long run, providing the homeless population with housing is the cheaper option to society. Also, as examined earlier, if applied in America, this Housing First policy will inevitably save more lives, with fewer interactions between the homeless and the police.
While homelessness is not something people are normally born into, the unhoused face discrimination, stigmatization, and marginalization from society just as much as any other group. Although people’s socioeconomic status is a major factor in determining who is most vulnerable to experiencing homelessness, as we’ve seen in the case of the LGBTQ+ youth, and older veterans as well, homelessness can impact people of any and all races, at various age levels, and at any given time. The pandemic itself has expanded the homeless population as people are unable to pay their backed-up rent or mortgage payments. While alternative approaches can assist to eradicate levels of homelessness in our society as implemented in Finland and Utah, it is crucial that we also continue to destigmatize being homeless in American society and take a rights-based approach to finding long-term solutions to end their suffering.
Justice and Love. Source: Renoir Gaither. Creative Commons.
On Tuesday April 6th, the Institute for Human Rights at UAB welcomed acclaimed author and activist Brittany Packnett Cunningham to speak. Brittany facilitated a conversation entitled “Pursuing Justice with Love and Power.” The discussion was moderated by IHR graduate assistant Jaylah Cosby and IHR intern Faiza Mawani.
Brittany began with discussing her inspiration for the phrase “love and power.” The phrase was actually borrowed from a lesser known piece of writing by Dr. Martin Luther King, Jr. It can be utilized in word format or in a series of emojis: the heart emoji to represent love and the fist emoji to represent power. Love and power are conceived as two opposites. For example, love is perceived as soft whereas power is perceived as intense. However, Brittany emphasizes the importance of the two together. Our power can be informed with our love. This can be seen in a political landscape with loving policies that empower people where they are.
Brittany then pivots the conversation to discuss love and power in the context of community building. Community building begins first by being in and participating in the community. She describes 2014 as a pivotal turning point in American history and in her personal history. With 2014 came the protests in Ferguson where young people protected the American people’s right to protest. Communities showed their love for themselves and for others by standing up to the injustices in local, national, and international communities. Love is the root of protests. Brittany states, “We don’t need to know the people who have died by police violence to love them.” To actualize what love looks like, it is required to be in community with people.
When asked about whether the term “community” can mean an integrated community or a homogenous community, Brittany confirmed that both are necessary in making sense of our racial identity in the world. Affinity spaces allow for safety and comfort in what we know and understand. Finding community in those affinity spaces often provides the opportunity to find community in multicultural spaces. While working towards that multicultural community can be difficult and uncomfortable, that safe space from the homogenous group is still there at the end of the day. In answering this question, Brittany emphasizes the need to push for integrated spaces while also understanding the simultaneous need for affinity spaces.
In the time of COVID-19, digitalization has become ever more present in all spaces an advocacy is no exception. Brittany acknowledges how digital spaces have somehow made it easier to work as an activist. She describes digitalization as another tool in the toolbox that works toward justice. It changes the way people can view work, life, and accessibility. However, the digitalization of life and work has also allowed misinformation to flourish. Brittany’s example of the dangers of misinformation is with voter suppression. The most effective form of voter suppression is to convince voters to stay home by encouraging them to believe that their vote doesn’t count. Similarly, Brittany warns against performative digital advocacy. If an Instagram post is being created with the sole purpose of gaining followers, this is an example of performative digital advocacy. Instead, advocacy posts should encourage action and therefore be productive. Most importantly, digital advocacy must amplify the folks most affected by the issue whenever possible.
A question from the audience inspired Brittany to discuss the intersection between religious faith and social justice. In response, Brittany stated, “I identify as political not in spite of my faith but because of it.” Brittany speaks from the perspective of a Christian and highlighted many of the issues modern Christianity has.
The conversation began to orient towards the Derek Chauvin case, which was ongoing at the time of the event, and policing in the United States. Brittany admitted to not watching the trial but looking at the coverage after the fact. Her primary reason for doing so is an understanding that nothing in the Derek Chauvin trial will bring back George Floyd. She highlights the important difference between justice and accountability in this section of the conversation. Justice would be an anonymous, alive, George Floyd sitting with his family and friends and living his life. That will never happen due to the actions of Derek Chauvin. However, Chauvin can be held accountable for his actions. When discussing the trial, Brittany states how she hopes that from the spectacle that is the trial, people are able to understand that police officers should never be expected or allowed to be the judge, jury, and executioner.
Brittany’s perspective on policing in the United States is that it needs to cease to exist how it is. She cites the “abolitionist tradition” of the United States. The people who fought against the abolition of slavery often argued the economics of slavery and the reliance the United States had on it, a similar argument we see occurring now when discussing police systems. Brittany asks the audience that if reimagining what public safety looks life scares you, to ask yourself where you would have stood on the abolition of slavery. “The safest communities,” Brittany states, “are not those with the most cops, both those with the most resources. Period.”
Brittany ended the conversation with advice on how to “get on the train” of activism. She says that the most important things to do are to listen, learn, and act but acknowledges that the temptation in activism is to default to whichever of those three is your are comfortable with, which is often “learn.” Brittany explains that it is easy to fall into the trap of sitting in the corner of your house, reading the literature and listening the people but never exiting to help build the communities and act. Learning is only half of the work. With such a digitalized world, there is an opportunity to learn and listen from the people we are the least like. Brittany advises to write down what gives you a privilege and an advantage in the world and follow the people who do not have your privileges. She also advises to act locally, highlighting the fact that you do not have to travel to another place to be an activist. “Link up with the organizations in your community,” Brittany advises, “and that is how we get to work.”
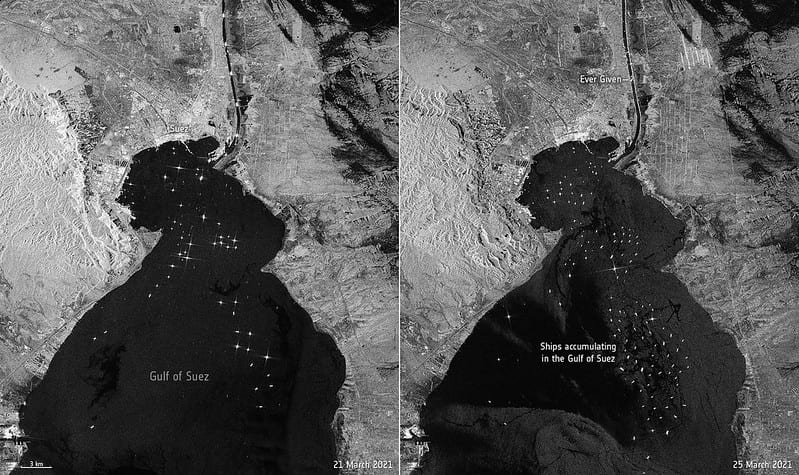
Every significant economic market in the world has a large reliance on the global supply chain, or globalization. These supply chains rely on canals to connect one side of the world to the other, including the Panama Canal and the Suez Canal. On Tuesday March 22nd, one ship single handedly disrupted the entire global supply chain. The Ever Given, one of the largest container ships in the world, ran aground in the middle of the Suez Canal. This event blocked any other container ships from crossing the Suez Canal in either direction, effectively cutting off a major link between Asian markets and European markets.
The blockage created by the Ever Given as of March 21, 2021. Source: European Space Agency. Creative Commons.
According to an analysis by Bloomberg, the Suez Canal blockage created by the Ever Given is holding up $9.6 billion of goods. Some blocked ships are carrying oil, others are carrying items from electronics to clothes. Should the blockade in the Canal last for two weeks, nearly one-fourth of the container ships that would normally be in European ports will be blocked. Normally, approximately 12% of global trade passes through the Suez Canal. Every day, the canal is able to move about 106 large shipping containers between Asia and Europe. To put this in perspective, before it was released, it is estimated that the Ever Given was holding up about $400 million an hour.
The world has recently been relying on markets that reduce the need for stockpiling items and instead provide products “just in time.” The internet and the current system of global shipping allow companies and consumers to buy and receive products right when they need them, instead of stockpiling. The COVID-19 pandemic provided a fantastic example of how “just in time” manufacturing has major flaws. From toilet paper to essential medical protective gear, certain products were in very high demand around the world. There was the assumption that these products could be delivered quickly and dependently to those who needed them at the start of the pandemic. However, this calculation was severely flawed and the high demand from all corners of the world for the same products caused months of delays in manufacturing leading to deadly consequences.
The Suez Canal. Source: David Reid, Creative Commons.
The Suez Canal runs through Egypt, connecting the Mediterranean Sea to the Indian Ocean. The canal was initially owned by French investors when it was conceived in the mid-1800s. The construction of the canal began in 1859 and took 10 years and 1.5 million workers. These workers were drafted from Egyptian peasants, approximately 20,000 peasants every 10 months, for extremely difficult work that was very poorly compensated. Many of these workers died of various diseases, including cholera, during their time working on the canal. Throughout the World Wars, Britain controlled the canal. However in 1956, British powers withdrew after many years of negotiating with Egypt. At that point, the Egyptian government led by President Gamal Abdel Nasser had control of the canal. The Suez Crisis began in 1956. Nasser had decided to nationalize the canal once the British forces departed. Israeli, British, and French forces decided to stage a military intervention after deciding the Egyptian response to the canal could be seen as a security threat. The crisis ended in 1957 due to the first-ever United Nations’ peacekeeping force.
The Suez Canal blockage created by the Ever Given has brought to light how much the world relies on cargo ships. 90% of the global trade is carried out within maritime supply chains. As the COVID-19 pandemic has continued, thousands of workers on ships have been stranded due to COVID-19 restrictions, unable to return to home countries and unable to be relieved. This has become a humanitarian crisis. Seafarers are the ones providing the world with food, essential supplies, and any other items purchased by consumers. However, they have been unable to leave their ships and go home to their families.
Cargo Ship. Source: Pedro Szekely, Creative Commons.
Crews on the ships are supposed to rotate on and off the vessels every 11 months. However due to the pandemic, many seafarers have long surpassed this 11 month marker and still have no notice as to when they can return home. Even before the pandemic, seafaring is a difficult job. The shifts are long, sleeping quarters are tight, and there is very little contact with those off of the ship. At the beginning of the pandemic, the situation was even described as bordering on forced labor. A major problem is the growing levels of fatigue experienced by the crew on ships. The number of reported suicides within this population has doubled, with this statistic not including the cases that were deemed accidents or missing at sea.
While the blockage of the Suez Canal by the massive ship, the Ever Given, has prompted memes and jokes around the world, it has brought more attention to the world’s reliance on shipping industries and to the lack of welfare experienced by seafarers. The Ever Given rendered the Suez Canal virtually useless for many days and the ramifications of this will fall primarily on the backs of shipping industry workers. It is important to recognize how COVID-19 has impacted the global economy as well as seafarers and to work towards achieving fair rights for these workers.
Swastika flag at a neo-Nazi rally in Massachusetts, USA. Source: Elvert Barnes, Creative Commons.
Hate symbols are hiding in plain sight. They are used to send messages, intimidate, and represent alt-right, white supremacist groups. Pretty much everyone around the world is able to recognize the swastika as a symbol of oppression and hate. However, hate groups have recognized how the swastika withdraws an immediate response of disgust and criticism from society. Therefore, hate groups have evolved to utilize symbols that perpetuate a very similar type of racism and hate as the swastika but are subtler and not as recognizable. Because of this, hate groups have been able to mobilize, protest, and distinguish their members from others without fear of retribution aimed at their symbols. This article serves as a baseline explanation of popular hate symbols within hate groups with the goal to make these symbols more recognizable and therefore less powerful.
People who utilize hate symbols in modern times work to ensure their ideologies are recognizable to likeminded people but not recognizable to the point that they might be criticized. Most of the time, neo-Nazis have three reasons to use a hate symbol: 1. They want to openly announce their support of the group/ideology 2. They want to intimidate or 3. They intend the symbols to be messages to other neo-Nazis. An example of secret messages would be the use of the number “1488.” 14 refers to the 14 words of a slogan utilized by white supremacists and 88 refers to “Heil Hitler” with H being the 8th letter in the alphabet. A popular way of hiding this message in social media posts, pieces of clothing, or on posters is to represent it on a pair of dice.
The Sonnenrad. Source: ADL, https://www.adl.org/education/references/hate-symbols/sonnenrad
The sonnenrad, or black sun, has long been a symbol of the neo-Nazi movement. While the symbol originates from an ancient Norse representation of the sun, more modern context shows us how the sonnenrad was a symbol of Hitler’s SS and after the fall of the Nazis in Germany, a symbol of the remaining Nazi supporters. Many hate symbols, including the swastika, have been appropriated from ancient cultural symbols in order to encourage dangerous racist narratives. The head of the SS, Heinrich Himmler, had a sonnenrad mosaic installed in the floor of the SS headquarters and included the SS’s insignia within the sonnenrad to represent the “Aryan race” the Nazis were intent on creating. Contemporary neo-Nazis have revived the symbol. While the swastika is known around the world as a hate symbol and is illegal in certain countries, the sonnenrad is not so well known despite the similar hateful connotations it represents. A manifesto created by Brenton Tarrant displayed the sonnenrad prominently on the cover. In March of 2019, Tarrant massacred 51 members of two Christchurch mosques. The sonnenrad has become alarmingly disseminated, with the symbol being used in memes and social media posts in support of alt-right leaders around the world.
The combination of the colors red, white, and black is another example of a neo-Nazi symbol. These colors were originally the colors of the German Empire that fell after World War I. Hitler deliberately used these colors when creating the Nazi flag, using propaganda and the colors to try and draw Germans into the Nazi agenda by connecting the imperialism of the German Empire and the Nazi regime. Hitler himself stated that the red represents the “social idea of the movement,” the white represents the movement’s roots in nationalism, and the black is for the swastika, or “the mission of the struggle for the victory of the Aryan man.” Since Hitler, neo-Nazi groups have revived the hateful symbolic meaning of the colors, strategically placing them to show allegiance to white nationalist ideologies.
Here is a short list of other common hate symbols:
A white nationalist group named the Detroit Right Wings claimed and altered the logo of the Detroit Red Wings. The altered logo contains a Nazi SS symbol, the sonnenrad, and prints it on shields and t-shirts.
The Valknot. Source: ADL https://www.adl.org/education/references/hate-symbols/valknot
The valknot, or “knot of slain,” is an ancient Norse symbol used to represent the underworld. This symbol has also been appropriated by white supremacists. These groups use the valknot to demonstrate a connection to ancient Nordic culture and in some cases to represent their willingness to die in battle for Odin, a Norse god.
The kekistan is an almost exact replica of the Nazi war flag, with the Kekistan logo replacing the Nazi swastika and the color green replacing the large swath of red originally found on the flag. It is the national flag of a fictional place, used to show allegiance to the alt-right and many of Hitler’s ideologies.
White Power hand gesture. Source: ADL, https://www.adl.org/education/references/hate-symbols/okay-hand-gesture
The “OK” hand gesture was once an innocent gesture used in general society as a gesture to mean “okay,” incorporated in American Sign Language, and utilized in Hindu and Buddhism as a symbol of “inner perfection.” However, starting in 2017, the symbol started being used to represent white power. It is flashed in social media posts and videos, most infamously used by Brenton Tarrant. Tarrant flashed the symbol in a courtroom in 2019 after being arrested for murdering 50 people at mosques in New Zealand.
Vanguard America, a prominent white nationalist group, uses the phrase “blood and soil” as an alt-right nationalistic slogan. In this context the definition is not far removed from the Nazi definition, just more directed towards the United States instead of Germany. The soil refers to “american soil” with blood referring to “white blood.” The phrase attempts to draw hereditary connections between the land of the United States and white people, completing negating the fact that many indigenous peoples lived and survived on the land of the United States for centuries before white people dared to grace the land with their presence.
The Nazi Iron Cross. Source: ADL https://www.adl.org/education/references/hate-symbols/iron-cross
The Iron Cross was a German military medal that has centuries of history. However, the Nazi regime claimed the medal and utilized it, placing a swastika within the metal of the cross, thereby making it a Nazi symbol. After World War II, the Iron Cross was primarily discontinued, however white supremacists, alt-right groups, and neo-Nazis have continued to use the Iron Cross as a symbol for their racist beliefs.
The Nationalist Socialist Movement (NSM) is one of the largest neo-Nazi organizations in the United States. The group is not shy about their respect and support for Adolf Hitler and will go so far as to wear Nazi uniforms with swastika armbands to protests. This group has roots in the American Nazi Party, founded in 1959. The NSM chose the Othala Rune as the new sign of alt-right white supremacy. The Othala Rune was originally an ancient symbol rooted in ancient Germanic cultures. It was appropriated by the Nazi movement in Germany to represent the “pure Aryan race.” It was chosen by the NSM after they felt the swastika was too recognizable and wanted something “more mainstream” to take on a very similar meaning as the swastika.
On January 6th 2021, the United States saw an attempted coup occur as supporters of former President Donald Trump stormed and raided the Capitol Building. Many of the symbols discussed above were prevalent on t-shirts, hats, and even skin. The QAnon supporter Jake Angeli, whose picture has been widely circulated since the event, had a variety of alt-right hate tattoos, including the Valknot. The neo-Nazi symbols themselves were enough to stem the rumors that anti-facist groups like ANTIFA were responsible for the attempted coup. However, outside of scholarly news articles, there was not much discussion about the symbols seen on flags, clothes, and skin on January 6th. In the case of modern hate symbols, their relative secretiveness gives them power. It is important to be able to recognize these symbols to keep marginalized groups safe and to hold people accountable who may support the meanings behind these symbols. For more information on the symbols outlined above and others, visit the ADL Hate Symbols Database.
An infographic displays the treatment of children by the authorities. Source: Yahoo Images.
The Human Rights Watch collected evidence in between January and June 2020 that closely reviewed the trial cases of 75 alleged child offenders who were recruited by the Islamic State (ISIS). The cases had led to the misconstrued holding of the children, but upon review, the Human Rights Watch ordered the release of the children, using reasons like a lack of evidence and preventing double jeopardy, as well as provisions of Iraq’s amnesty law. The 2016 Iraq Amnesty Law offers amnesty to persons who can show that they joined ISIS or another terrorist group against their will and did not commit a serious offense prior to joining the group.For years, Iraqi and Kurdistan judicial authorities have charged hundreds of children with terrorism for alleged ISIS affiliation. Several of the charges have been based on the dubious accusations and forced confessions of these children, regardless of the extent of their involvement with ISIS, if any. Such behavior from authorities has led to an international norm that children recruited by armed groups should be treated as victims, first and foremost, not as criminals.
In January 2020, a committee formed under the Nineveh Federal Court of Appeal and Bar Association, consisting of a judge, a general prosecutor, and a social worker. This committee adjudicated the cases of suspects who were children at the time of their alleged alliance with ISIS. The approach taken by this committee was one of compassion and complied very well with acknowledging the human rights of these child suspects. In June 2020, Iraqi judicial authorities dissolved the committee, saying it had reviewed all the pending cases, but another committee in Nineveh, Iraq, continued adjudicating such cases. In August 2020, an anonymous source close to the Nineveh Bar Association told the Human Rights Watch that the committee had reviewed 300 case files before being disbanded in June. They convicted 202 people, dropped charges against and released 31, and pardoned and released 44 under Iraq’s 2016 Amnesty Law. Three cases were dropped because the defendant had already served a sentence for the same crime, so to not invoke double jeopardy, the committee permanently ceased proceedings against the three people.
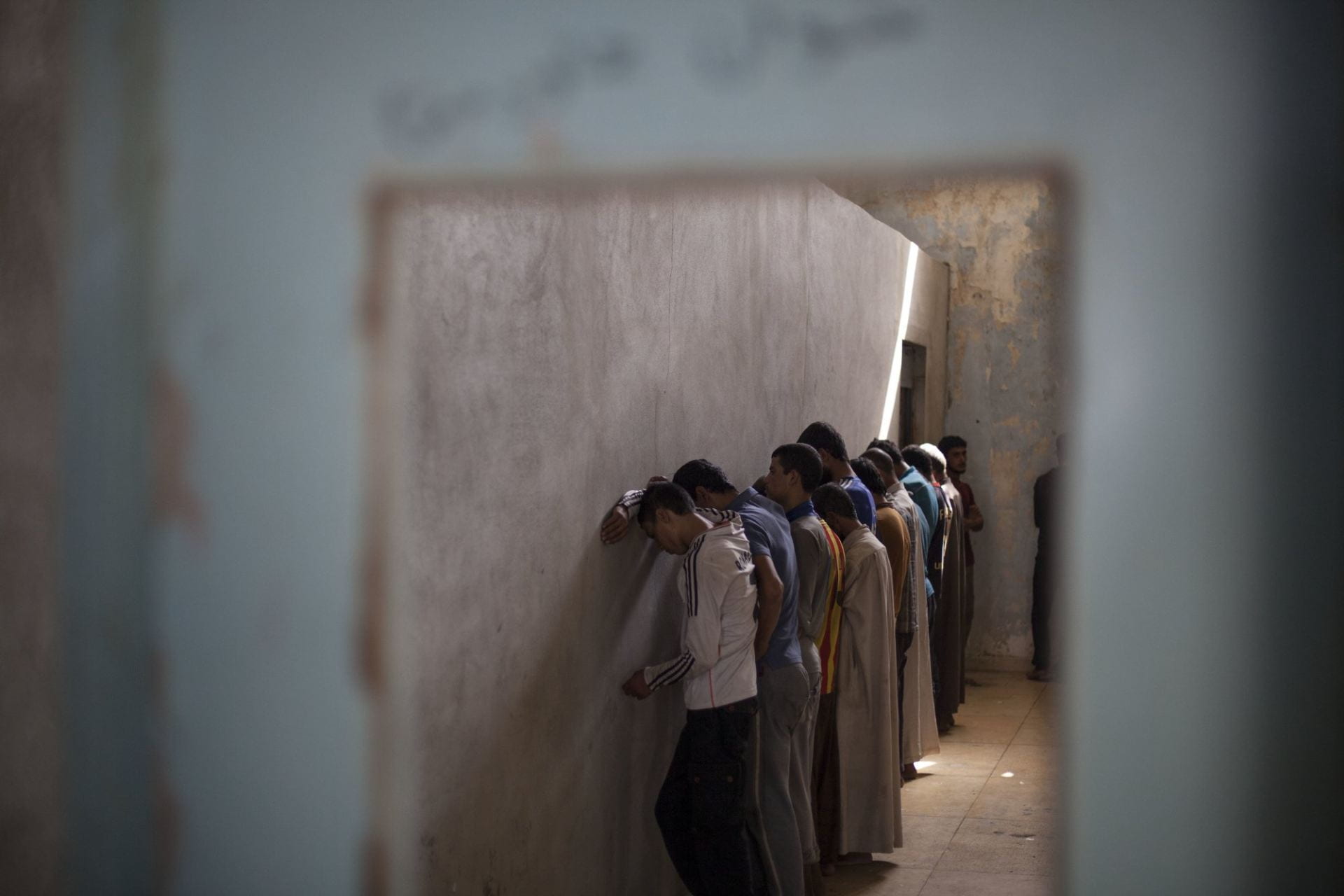
Arrested child suspects line a corridor, awaiting response from the police. Source: Yahoo Images.
The committee, unlike other Iraqi courts, attempted to review individual cases more fairly and better apply international standards. By doing so, it was able to convict the guilty and release the innocent, which Iraqi courts do not have the best record for. In the Iraqi-Kurdistan regions, children have been tried in Kurdistan and re-tried for the same crime in Baghdad-controlled territory, with courts ignoring whether or not the child had been acquitted or convicted and already served a sentence in Kurdistan.
This has been the case since the advent of ISIS in Iraq: hundreds of children have been charged with crimes of terror, and such convictions have been justified under Iraq’s 1983 Juvenile Welfare Act. The Act states that the minimum age of criminal responsibility is 9 in Iraq and 11 in the Kurdistan region. Children that are under 18 at the time of the alleged crime are sent to a “youth rehabilitation school” which is designed to provide social rehabilitation and reintegration via educational or vocational training. However, a source within the Tal Kayf prison said that “the cells are identical to those for adult detainees, with no access to any reading or studying materials besides the Quran.”
What needs to be done?
The Nineveh committee is the first step towards attaining a more efficient and fair judicial system in Iraq where ISIS affiliation does not automatically translate to imprisonment. Children should only be detained as a last resort and for the shortest appropriate period, in compliance with international law. Countries should provide proper assistance for children illegally recruited by armed groups and/or forces, including assistance for their physical and psychological recovery and social reintegration. The Iraqi government and Kurdistan Regional government should amend their counterterrorism laws to end the detention and prosecution of children solely for participating in ISIS training or membership with recognition of international law that prohibits recruiting children into armed groups. And the High Judicial Council should permit committees to delve into more counterterrorism cases to avoid the trend of double jeopardy, while instructing judges across Iraq to release all children who have not committed crimes and ensure their proper rehabilitation and reintegration.
In the first half of 2020, Iraq has taken an essential step towards protecting the rights of children rather than trampling them. But this progress is at risk of Iraqi officials do not implement such steps elsewhere.
One of the best things that my 12th grade high school teacher encouraged me to do was to read and watch Just Mercy, a book written by Bryan Stevenson and a film directed by Destin Daniel Cretton. Both the film and book allowed me to greater understand the importance of confronting injustice, while also standing up for those wrongly convicted.
The death penalty has been present in societies for hundreds of centuries, dating all the way back to before the establishment of Hammurabi’s Code in 18th century BC. Hammurabi’s Code laid the foundation of the death penalty for 25 different crimes; placing emphasis on theft between two groups of people. Hammurabi’s Code also established punishment as equal to the crime committed, as known from historical references as “an eye for an eye, and a tooth for a tooth.” These types of punishments were often cruel and included crucifixion, burial alive, impalement, and others.
The Guillotine, one of the older methods of execution, was introduced in France in 1792. This device fixes the head between two logs with a heavily weighted knife suspended a couple of feet in the air. This method of execution was introduced to make the process of execution “by means of a machine,” making it “as painless as possible.”
Carried out in countries in Asia, North Africa, and the Middle East, hanging is defined as suspending someone in the air as a form of execution. Death either occurs through decapitation or through strangulation, depending on the length of the rope compared to the weight of the prisoner.
Lethal Injection
Lethal Injection consists of an anesthetic alongside chemicals used to paralyze the prisoner and stop the heart. This form of punishment exists in China and Vietnam.
Surprisingly, the United States also uses the lethal injection, with the most recent execution taking place on September 24th, 2020. “Christopher Vialva was sentenced to death for the 1999 murders of Todd and Stacie Bagley.” Vialva’s execution was the 1,526th in the United States since 1976, 10th in the federal system, and the 1,346th person executed by means of lethal injection.
Although the injection is designed to kill ‘quickly’ and ‘smoothly,’ inexperience on the part of prison staff has flawed the execution process. One case in particular is that of Dennis McGuire. Reports show that after the injection was administered to Dennis McGuire, he gasped and convulsed for 10 minutes; much longer than the time that previous injections have taken to execute someone, before dying.
Electrocution
Execution by electrocution occurs when a prisoner is strapped to an electric char with a “metal skullcap-shaped electrode” attached to their scalp or forehead. Following these actions, the prisoner receives a jolt of electricity up to 2000 volts for up t o30 seconds, until the prisoner is dead.
Electrocution is a method of execution carried out in the United States, with the first electrocution taking place at Auburn Prison in New York against someone who was convicted of murdering “with an axe.”
Why the Continuation of the Death Penalty Creates a Gray Area
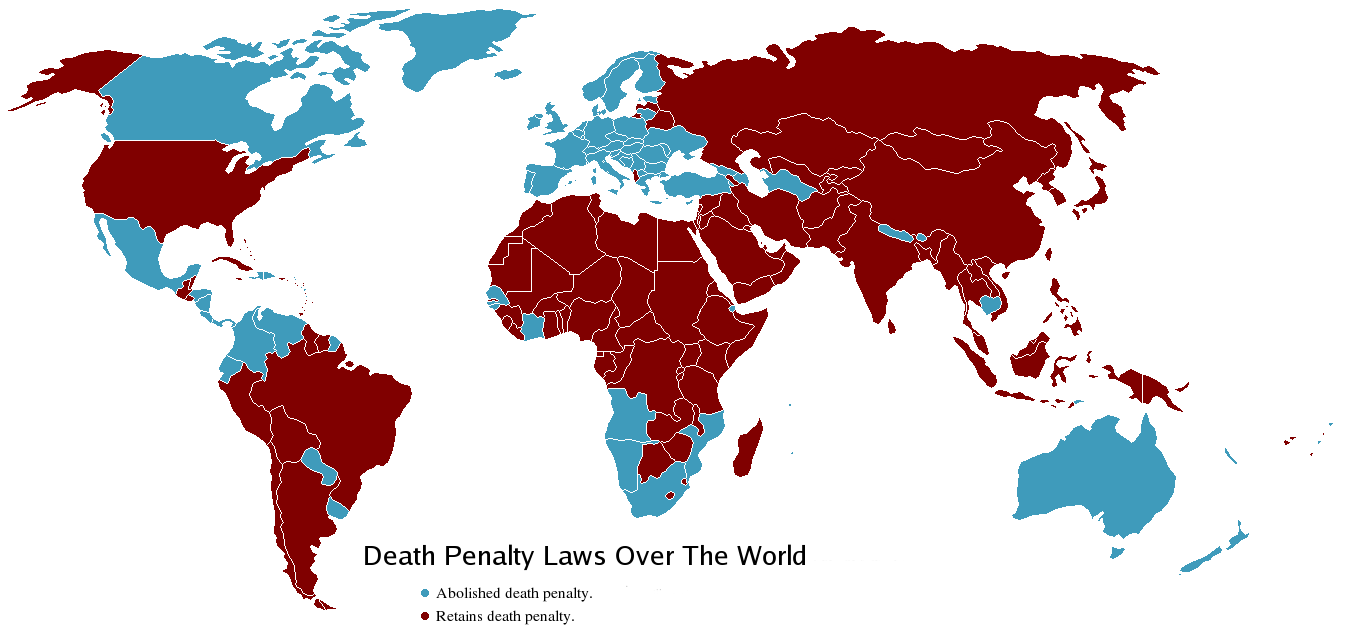
According to the Embassy of the United States of America, capital punishment still exists due to the inability of the federal government to dictate laws to the states. Although the United States has been one of the foremost leaders in reforming capital punishment, other countries have had an easier time in abolishing it by “national governments imposing top-down reform because they decided the death penalty was no longer necessary or legitimate.” And since the Constitution allocates criminal law to the states, only they can repeal their own capital punishment laws. The Supreme Court is the only national-level body capable of declaring capital punishment unconstitutional.
Around the world, many consider implementing the death penalty a violation of human rights, especially those that require states to recognize the right to life, as shown through Article 3 of the Universal Declaration of Human Rights: “Life is a Human Right.” Although intended to curb violent crimes and atrocities committed by criminals, the loss of life through the death penalty violates “the right of life and the right to live free from torture or cruel, inhuman or degrading treatment or punishment,” which the death penalty unfortunately promotes.
Although many international organizations and countries have abolished the death penalty, like many countries of the Global North save the United States, a case can arise where the death penalty is justified, shown through Bangladesh’s approval of the death penalty for rape. With a viral video showing a group of men sexually assaulting a woman, Bangladesh’s cabinet quickly approved “to incorporate the death penalty for all of the four types of rape defined under Bangladeshi law.” Though detracting from the real problem, that rapists are normal people and not animals, the passage of the death penalty seems just, since there has been a violent outrage at the lack of enforcement on sexual violence in this part of the world.
Moral arguments for the death penalty put quite simply, is the concept of retribution, where the killing of one person justifies the death of the killer. However, opponents of this notion would counteract that point with the fact that issuing capital punishment detracts from the moral message it conveys, alongside the fact that it is fundamentally inhumane.
Despite these arguments, the inhumane action that is the death penalty cannot go unchecked. With the death of Dennis McGuire, for instance, these processes are not clean and fraught with mistakes leading to the disgusting and horrific death of inmates.
“The death penalty has no place in the 21st century” – António Guterres
Overall, the “death penalty is not a useful instrument for combating crime.” Abolishing the death penalty in the United States can allow other countries to ensure the right to life for all people, while also ensuring that the absolute worst of punishments cannot be enforced differently based on a person’s status, color, race, or underlying distinctions.
“The death penalty is the ultimate cruel, inhuman and degrading punishment.” – Amnesty International
UAB is an Equal Employment/Equal Educational Opportunity Institution dedicated to providing equal opportunities and equal access to all individuals regardless of race, color, religion, ethnic or national origin, sex (including pregnancy), genetic information, age, disability, religion, sexual orientation, gender identity, gender expression, and veteran’s status. As required by Title IX, UAB prohibits sex discrimination in any education program or activity that it operates. Individuals may report concerns or questions to UAB’s Assistant Vice President and Senior Title IX Coordinator. The Title IX notice of nondiscrimination is located at uab.edu/titleix.