The Kenya Girls Guide Association hosted a rally against FGM during 16 Days of Activism in 2011. Source: Yahoo Images
The killing of Corporal Mushote Boma on December 15, 2023, in Elgeyo Marakwet County, Kenya, has brought to light the deeply entrenched issue of female genital mutilation (FGM) and the urgent need for increased awareness and action to eliminate this harmful practice. The tragic incident, where Corporal Boma was stoned to death by a mob of young men after rescuing a group of girls who had been forced to undergo FGM, signifies a significant setback in the fight against this violation of human rights in Kenya.
Female genital mutilation, also known as female genital cutting or female circumcision, is a practice that involves altering or injuring the female genitalia for non-medical reasons. FGM is a harmful practice and a violation of the rights of girls and women. It can lead to severe physical, emotional, and psychological consequences, including but not limited to severe bleeding, infections, complications during childbirth, and long-term psychological trauma. The World Health Organization (WHO) has classified FGM into four types, with type 3 being the most severe, involving the removal of all external genitalia and the stitching of the vaginal opening.
According to reports, the incident involving the Corporal occurred when the police were taking the rescued girls to the hospital after the illegal FGM procedure. It is a grim reminder of the challenges faced by law enforcement officers and activists in combating such deeply rooted harmful practices. Despite the ban on FGM in Kenya, the practice still persists in certain areas, often conducted during school holidays, using crude methods and tools by individuals who continue to defy the law.
It is essential to understand that the practice of FGM is not limited to Kenya but is prevalent in many African countries, as well as in some parts of Asia and the Middle East. The complexity of cultural, social, and traditional beliefs and practices surrounding FGM makes the fight against it particularly challenging.
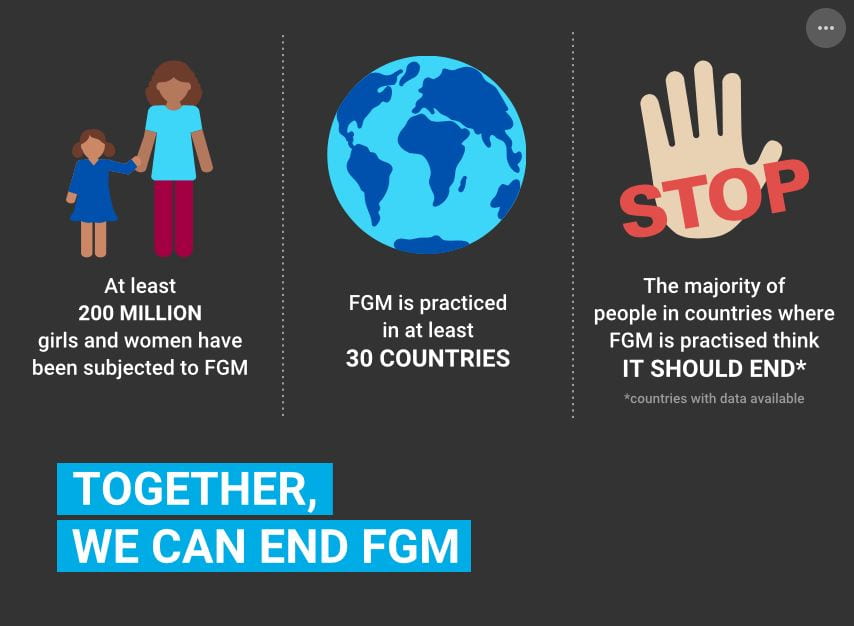
An infographic on FGM, including information about how many girls and women are impacted by it, is practiced in over 30 different countries around the world. Source: Yahoo Images
In the wake of Corporal Boma’s tragic killing, there is an urgent need for heightened awareness and education about the dangers of FGM. The involvement of communities, religious leaders, and other stakeholders is crucial in effectively addressing and eliminating this harmful practice. There is a pressing need for community-based interventions focused on education, awareness, and empowering women and girls.
Furthermore, it is imperative for the Kenyan government and other relevant authorities to take decisive action and strengthen the enforcement of laws against FGM. Perpetrators of FGM must be brought to justice to send a clear message that this harmful practice will not be tolerated in any form. The government should collaborate closely with local organizations and international partners to develop and implement comprehensive strategies to combat FGM effectively.
The media can play a pivotal role in raising awareness about FGM and shaping public opinion on the issue. Media campaigns and educational programs can provide crucial information on the physical and psychological consequences of FGM, dispel myths and misconceptions, and promote positive social norms around the issue. Additionally, the media can highlight success stories of communities that have abandoned the practice of FGM, inspiring others to follow suit.
At the global level, the international community plays a vital role in supporting efforts to combat FGM. International organizations, including the United Nations and its specialized agencies, as well as non-governmental organizations, have been advocating for the elimination of FGM through various programs and initiatives. These efforts range from providing direct assistance to affected communities, conducting research and data collection, advocating for policy changes, and supporting grassroots organizations working at the local level.
Some resources are laid out for community members to learn about the dangers of FGM. It includes pamphlets, brochures, and a 3D model used to teach about different types of FGM. Source: Yahoo Images
The killing of Corporal Mushote Boma serves as a stark reminder of the urgent action needed to eliminate the harmful practice of female genital mutilation. It is crucial to work collectively to raise awareness, educate communities, and enforce laws to protect the rights of girls and women. This tragic incident must galvanize individuals, communities, and governments to address FGM comprehensively and put an end to this barbaric practice.
The world must unite to protect the rights and well-being of girls and women globally and ensure that no one else suffers the same fate as Corporal Mushote Boma. By fostering a culture of respect for human rights and gender equality and by promoting positive social norms and behaviors, we can strive to create a world where every girl and woman has the right to live free from the fear and trauma of female genital mutilation. Together, we can work towards a future where every girl and woman can fulfill her potential without being subjected to the physical and emotional pain of FGM.
The tragic killing of Corporal Boma is a solemn call to action, and it must be responded to with determination, compassion, and unwavering commitment to bringing an end to the harmful practice of female genital mutilation once and for all.
*The use of gender-affirming language is incredibly important, and it is vital to remember that women are not the only people capable of giving birth or the only people subjected to maternal risks. Unfortunately, research on transgender, intersex, and nonbinary births is incredibly limited, so for the sake of concision, this post will refer to the maternal mortality crisis largely in the context of women. *
Maternal Mortality
Maternal mortality is perceived as a thing of the past. In the 21st century few feel as apprehensive about the idea of them or a loved one giving birth as they would have in centuries prior. One group that does not share this same luxury is black mothers. In America, black women are three times more likely to die from pregnancy-related causes than white women. Causing these issues are years’ worth of issues, including differences in the quality of healthcare, implicit bias, and structural racism.
With 80% of pregnancy-related deaths being preventable, it empowers no one to learn that Alabama is one of the greatest perpetrators of maternal mortality with the third highest rate in the country. A piece of anecdotal evidence that I stumbled upon while researching this topic is local to not only Birmingham, but to UAB as well. A former faculty member of UAB, Angelica Lyons, was subjected to pregnancy-related trauma that was, simply put, unnecessary and preventable. Lyons, after emphatically describing her symptoms to her doctors, was brushed off and the severity of her symptoms was not realized. Because of this neglect, she was forced to live with an undiagnosed case of sepsis that resulted in an emergency C-section months before her due date. Fortunately, both she and her baby survived although it was a close call for the Lyons mother. This is not an atypical experience for women of color, and black women specifically. Historical bias against black women results in many doctors dismissing their pain as typical or as something they can handle.
To understand the racism incorporated in the gynecological field, it is important to briefly address the history of gynecology. Gynecological science began in the 1840s, when J. Marion Sims, the so-called “father of gynecology,” performed experimental C-sections on black slaves without any anesthetics. This inhumane treatment continued after the abolition of slavery, with unnecessary hysterectomies being performed on black women. Dr. Deirdre Cooper Owens said it best when she stated, “the advancement of obstetrics and gynecology had such an intimate relationship with slavery, and was literally built on the wounds of Black women,” Following this, black families were kept from white hospitals with substantial funding until the Civil Rights Act of 1964. The Civil Rights Act did not completely eliminate the disparity, and healthcare discrimination still follows us to this day.
Photo of a University of Alabama at Birmingham building, displaying the words “University Hospital.” Source: Flickr
Maternity Deserts
One cause of inadequate care for all mothers is maternity deserts. Maternity deserts are counties that have no hospitals offering obstetric care, no birthing centers, and no obstetric providers. Over two million women between the ages of 15 and 44 live in these maternity deserts, and between 2020 and 2022, the number of counties determined to be maternity deserts increased. Maternity deserts disproportionately affect Black and Hispanic neighborhoods (although, this post focuses on black mothers, as the difference between black and white mothers tends to be starker). Maternity deserts often have lower access to transportation as well, and these transportation barriers can hinder the utilization of prenatal care.
Photo of an industrial city, featuring train tracks, cranes, and various types of buildings. Source: Flickr
A Broader Scale
Health disparities amongst black people are not isolated to maternal issues. Black people must struggle with medical practitioners throughout their entire lives. Doctors habitually brush away the concerns of black people of all ages, causing them to be misdiagnosed, and resulting in worse treatment than their white counterparts, or no treatment at all. As written about in this post, this begins when black people are in utero and can lead to lifelong health conditions that are misunderstood and under-addressed.
For example, black children are more likely to have asthma and less likely to have treatment. There are many reasons for this; however, I am choosing to focus on the long-term effects of Jim Crow laws. Unfortunately, many areas with below-average housing (or areas located near toxic sites) are the same areas that were the result of previous redlining. Comparatively, 4 in 10 black children live in areas plagued by poor environmental factors, as opposed to just 1 in 10 white children. People are quick to discount the social factors that play into conditions such as asthma; however, many scientists agree that structural conditions can worsen asthma and cause certain groups to be unable to obtain treatment.
Later in life, black people are more likely not only to have Alzheimer’s, but they are also less likely to be properly diagnosed, which delays or prevents their ability to get treatment (not dissimilar to the conditions referenced above). Statistically, black people who are over 65 are 4% more likely to have Alzheimer’s than white people (14% versus 10%), but it is likely that this disparity is even larger due to said misdiagnosis.
Photo of a blue inhaler. Source: Flickr
Progress
While black maternal mortality is still an incredibly pertinent issue, progress has been made in recent years. In 2019, two members of the House of Representatives, Lauren Underwood and Alma Adams, created the Black Maternal Health Caucus. This caucus is one of the largest bipartisan groups in Congress, and its goal is to “work with…partners in industry, nonprofits, and the Administration to find solutions to ending disparities and achieving optimal birth outcomes for all families”. One creation by the caucus is the Black Maternal Health Momnibus Act, or more casually, the Momnibus. The Momnibus aims to address the maternal mortality crisis through investments in every aspect that may exacerbate mortality rates. It includes 13 bills that aim to enlarge the perinatal workforce so that it addresses diversity needs, extend the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) eligibility so that mothers can have support for longer periods of time after giving birth, increase support for mothers who are incarcerated, invest in federal programs that benefit mothers and infants during public health crises, promote vaccination among mothers, and more.
Another move towards progress is with President Biden’s proposed 2024 budget. This budget incorporates $471 million in funding. One of the tangible things that it will include is Medicaid for twelve months postpartum. These efforts are admirable beginning steps; however, the work is far from complete.
An empty room with three windows, all with long, sheer curtains. The two ceiling lights are off. Nothing but light can be seen outside the windows. Photo by Hans Eiskonen on Unsplash.
Mental Health, Autonomy, and Psychosocial Disability
In 1887, Elizabeth Seaman—better known as Nellie Bly—published Ten Days in a Mad-House, a collection of articles she had previously written for Joseph Pulitzer’s New York World. Along with cementing her status as a World journalist, her raw, unfiltered reporting offered thousands of readers a rare glimpse into a mysterious frontier: American mental asylums.
A Pennsylvania native, Bly’s anonymous newspaper pieces championing women’s rights soon evolved into a career based on investigative journalism. However, complaints from her subjects resulted in newspaper executives assigning her to less controversial topics. After years of rejection and gender discrimination, Bly made a last-ditch attempt to save her career by approaching Pulitzer directly and weaseling her way into a novel undercover assignment. Critics had called her insane her entire life for her risky stories, and now she had to play the part.
Bly’s articles quickly garnered attention for numerous reasons. For one, the story itself was sensational. After successfully feigning insanity with odd mannerisms and facial expressions, Bly found herself in New York City’s Women’s Lunatic Asylum after a medical professional declared her clinically insane. There she remained for ten days despite immediately dropping the act. During this period, staff allegedly attributed her every move, including normal behavior, to her supposed mental illness. This would have perpetually prevented her release had outside contacts not stepped into vouch for her sanity. By this time, Bly had risen to minor celebrity as New York questioned where this “pretty crazy girl” had even come from.
Sanitation was poor. Disease was rampant. Food and potable water were scarce, and the staff frequently resorted to physical and verbal beatings when dealing with those under their care. Upon her exit, Bly stated that she believed many women there were as sane as herself. If anything, the asylum’s treatment of already vulnerable women caused insanity.
A dilapidated wooden shed with some white paint on the door and bottom boards. It has two windows with broken glass and rusty frames. Behind it its dense woods. Photo by Lilartsy on Unsplash.
Life in Mental and Physical Shackles
Despite Bly’s work sparking outrage over a century ago, inhumane treatment of those with mental health disorders—or psychosocial disabilities—continues today. According to the World Health Organization, 1 in 8 people live with mental health issues. Without adequate support and resources, these conditions can quickly become disabling. Psychosocial disabilities share strong correlations with higher poverty rates, increased medical discrimination, occupational inequity, and other factors contributing to a generally lower quality of life.
In 2020, Human Rights Watch released 56-page document reporting rights violations of the mentally ill. “Shackling,” a recurring theme, was found in 60 countries across six continents.
Shackling is an involuntary type of hyper-restrictive housing. Although it does not include shackles specifically, restraints such as ropes, chains, and wires are commonplace methods in keeping the victim in extremely close quarters. These areas can be sheds, closets, or even caves. Similar to the asylums in Bly’s era, sanitation is a luxury. The detained person often eats, drinks, and defecates in the same space with little ability to prevent contamination.
The motives and background around shackling is a complex cultural issue. Some offenders tend to be family members who, despite loving the person, lack the resources and/or education to deal with mental health crises. Keeping the person confined can appear to be the safest option when confronted with the possibility of them hurting themselves or others.
Additionally, social stigma can create even more danger for the family as a whole as well as the mentally ill individual. Instead of risking exile or ostracization from the community, families may seek alternative healing methods at home, such as herbal remedies, that lack significant medical backing. This, in turn, can intensify psychosocial disability, leaving the family overwhelmed and confused with few options.
A photograph of a medical IV stand holding and empty IV bag on a dark background. Photo by Marcelo Leal on Unsplash.
Abuse at the Systemic Level
However, abuse does not just occur at the familial level. Mistreatment and abuse flourish in large institutions. The institutions go by many names: asylums, mental hospitals, psychiatric healing centers, etc. These are establishments, often state-funded, purposefully keeping those with psychosocial disabilities away from the general population. Although the institutions usually operate under the pretext of healing and protecting the mentally ill, many criticize the asylum system for blatant human rights offenses.
Paul and his companions walked in chains—literal shackles—and were not allowed clothing. His restroom was a bucket.
In the USA, a wave of deinstitutionalization in the 1970s shuttered many mental asylums, and psychiatric facilities still operating do so with varying levels of success. New York City’s mayor Eric Adams recently announced an expansion of a law allowing months-long involuntary commitment to hospitals for those who, due to mental illness, failed to acquire “basic needs” such as shelter and food. Hospitalization would, in theory, provide the psychosocially disabled with the time and education to recover and start anew.
Opponents quickly pointed out flaws in this process.
As with shackling, involuntary hospitalization represents a loss of autonomy. In a 2022 article in The Guardian, Ruth Sangree reflects on the USA’s changing legislation by connecting it to her own experiences. She describes the monotonous isolation, undercurrent of fear, confusion resulting by the sudden loss of control over her own life. As a nineteen-year-old with no idea of when she would be “set free,” Sangree focused on appearing normal in fear of indefinite hospitalization, regardless of the effectiveness of treatments.
There stands the argument of many critics of institutions: the system is ineffective at best and traumatic at worst. Still, rebuttals exist. In one Times piece, retired employees from a California asylum vouch for the happiness of their patients, stating they “blossomed” when provided with regimen and shelter. This view forms the defense for New York’s law revision, which frames involuntary hospitalization as a compassionate action for the patient’s own well-being.
Objectively, both sides claim to want the same thing: a better quality of life for those with psychosocial disabilities. It has always been the how that stirs debate.
Eight people of varying skin and sleeve colors standing in a circle with one hand each stacked on top of each other’s. Photo by Hannah Busing on Unsplash.
The Future of Mental Health Care
One factor in the corruption of institutional systems lies in language. Terms like “healing center” and “asylum” have historically protected potential perpetrators from legal action. Nellie Bly’s work helped lift the veil around mental health and disability, peeling away the euphemisms to reveal the abuse of a vulnerable population.
Today, watch groups exist for this reason. Organizations such as the Alabama Disability Advocacy Program (ADAP) examine the care of people with disabilities in facilities like hospitals, nursing homes, and schools, where caregivers can easily take advantage of those under their care. If rights violations are found, they can work with the facility to improve conditions or take legal action. These organizations exist on a state and national level in the USA.
Individuals can make a difference by simply learning about mental health and advocating for equal treatment of those with mental health conditions. #BreakTheChains is a movement led by Human Rights Watch with goals of educating communities to prevent the chaining of men, women, and children with psychosocial disabilities.
Additionally, awareness is key—October is recognized as mental health awareness month, and invisible disabilities week is in late October. Psychosocial disability month specifically takes place in July.
November 10 is the International Day of Science and Peace (IDSP), also known as the World Science Day for Peace and Development. The United Nations host this international event.
History of IDSP
Established in 1986, this historical day was initially developed to commemorate the birth of Marie Curie, a notable physicist and humanitarian. Curie was known for her innovative work within radioactivity, contributing to the discovery of radium and polonium. By 1999, its purpose changed to reflect the global needs of the scientific and humanitarian community, utilizing the day to affirm the global commitment to attaining the goals of the Declaration on Science and the Use of Scientific Knowledge. The day and annual summit unite governmental, intervention mental, and non-governmental organizations meaningfully to promote international solidarity for shared sciences between countries and renew the global commitment to use science to benefit communities that need it most.
The 2023 theme for IDSP will be “Bridging the Gap: Science, Peace, and Human Rights.” This emphasizes the interconnectedness between science and peace, having a role in advancing human rights. Science is a valuable tool for making technological advancements, but it is also helpful in helping address social issues, reducing conflicts, and sustainably promoting human rights.
Photo of space shuttle near body of water. Source: Flickr
Science and Human Rights
Science is frequently associated with helping improve medical interventions, solving coding bugs, and completing mathematical equations. However, contrary to popular belief, science is essential to human rights. Firstly, science has a valuable role in promoting sustainable development. Utilizing scientific methods, data can be collected to quantify the progress toward fulfilling the 17 UN Sustainable Development Goals. Ranging from climate change to poverty to infant mortality, scientific data collection and analysis methods are needed to efficiently and effectively respond to global issues. Research and innovation also contribute to the mobilization of resources to historically underserved communities, allowing them to gain access to necessities.
Within innovation, shared desires and interests help unite countries with singular goals. Scientific diplomacy is valuable in bringing countries to the table of collaboration. This deepens connections between countries as it relates to trade and commercial interests and helps foster peaceful relationships, prioritizing human rights.
With the appropriate distribution of resources, scientific advancements help improve the quality of life for communities internationally. Applying what is traditionally “scientific” to communities gives them a chance to live a better quality of life in a cleaner environment.
It is available to educate the public about the vital role of science and encourage innovation to solve global challenges.
How Countries Can Get Involved
Beyond participating in IDSP, countries can have a role in unifying science and human rights through many different avenues. One route is to protect and invest in scientific diplomacy. By allocating funding to scientific innovation and multilateral collaborations, governments can ensure that they can focus on shared goals with their international counterparts, working collaboratively to promote peace and cooperation. Another route is developing policies that protect innovation while developing guardrails for its usage, ensuring it is mobilized to those who need it most. States have a responsibility to be an advocate and protectors of their citizens, and by working to ensure that scientific diplomacy is used for the betterment of people abroad, they can elicit change in a meaningful way.
INTL and MAST Students Visit US Department of State Source: GU Blog
How Citizens Can Get Involved
Citizens have a responsibility to promote peace with science, as well. The role of a community member is to primarily use one’s voice to advocate for innovation and peace; by doing so and mobilizing one’s own story, organizations are held accountable for their actions. From governmental entities, non-profit organizations, and grassroots movements, stakeholders are supported by the citizenry. It is also important to have open conversations to explore further the nuanced introspection of science, peace, and human rights, continuing to promote awareness and understanding.
What Are Institutions for People with Disabilities?
In this post, I focus on the institutions that were, and remain, facilities operating for the purpose of housing people with disabilities. The National Council for Disability (NCD) defines these institutions as “a facility of four or more people who did not choose to live together.” They summarize a report made by a consortium of self-advocacy organizations based on their experiences with institutionalization. The NCD list of criteria to define an institution, as synthesized from various self-advocacy groups, is that they:
Include only people with disabilities,
Include more than three people who have not chosen to live together,
Do not permit residents to lock the door to their bedroom or bathroom,
Enforce regimented meal and sleep times,
Limit visitors, including who may visit and when they may do so,
Restrict when a resident may enter or exit the home,
Restrict an individual’s religious practices or beliefs,
Limit the ability of a resident to select or remove support staff,
Restrict residents’ sexual preferences or activities,
Require residents to change housing if they wish to make changes in the personnel who provide their support or the nature of the support,
Restrict access to the telephone or Internet,
Restrict access to broader community life and activities.
Historically, these kinds of institutions have primarily included people struggling with mental health and people with intellectual or developmental disabilities.
What Were America’s First Institutions for People with Disabilities?
Mental institutions in America predate the reality of an American nation. The earliest hospital for the mentally ill, the Publick Hospital for Persons of Insane and Disordered Minds, was founded in Virginia in 1773. It was closer to a prison than what we would now call a hospital; patients were kept chained and shackled, physically abused, intentionally fed rotten food, and bathed in ice water. Inmates were rarely released. Many were placed or kept in prisons prior to or after their evaluation as being “insane.” This began to change in the 1840s; a new medical director attempted to use more humane approaches to treatment. Those included treatment that was consented to and largely removing chains and shackles.
The first modern institution for disabled people was founded by Samuel Gridley Howe in 1848 in Boston, Massachusetts. It was considered experimental, despite others’ previous endeavors taken elsewhere, but Howe had experience in a similar environment, having founded the Perkins Institution for the Blind twenty years earlier. A contemporary article sings praises of the institution. Despite that, the electronic catalog of annual reports by the institution, renamed the Walter E. Fernald State School, ends abruptly in 1973 with a report on identifying child abuse and neglect.
Small Victorian-era prison cell. Source: Yahoo Images
John F. Kennedy
John F. Kennedy (JFK) played an important role in the early reform of institutions for people with disabilities. Many people know that Kennedy’s sister, Rosemary, was lobotomized, leaving her permanently disabled and confined to a psychiatric institution. Lesser known is that Kennedy established the President’s Panel on Mental Retardation in 1961, the first government committee on the topic. The committee’s recommendations led to numerous regulations being changed and legislation being passed. One Panel member, Eunice Shriver, who was also Kennedy’s sister, went on to found the Special Olympics.
Institutions for People with Disabilities in Alabama
The first mental hospital in Alabama was the Alabama Insane Hospital, founded in 1859 and renamed to Bryce Hospital in 1900. Ricky Wyatt, at the time 15 years old, was committed by a court to Bryce in 1969. He was not mentally ill.
Wyatt’s institutionalization led to a widespread deinstitutionalization movement. His guardian, a former employee of the hospital, sued Bryce Hospital on his behalf. During the discovery process, Wyatt’s lawyers discovered numerous preventable deaths in the facility, as well as a complete lack of plans in case of a fire; there was no way to contact the Tuscaloosa fire department after 5:00 PM, and the fire hydrants on the property were decades old and incompatible with modern firefighting equipment.
That lawsuit, Wyatt v. Stickney (1972), was part of the beginning of a legal deinstitutionalization movement. It created a minimum standard for care at Alabama institutions for the mentally ill.
Willowbrook State School
Willowbrook was a state-funded institution in Staten Island from the 1940s until the late 1980s. The school was over its capacity in only a few years; in 1965, Robert Kennedy described Willowbrook as a “snake pit” with “rooms less comfortable and cheerful than the cages we put animals in a zoo.” The few changes that resulted from Kennedy’s visit were insubstantial and short-lived.
Another infamous incident in Willowbrook’s history was the hepatitis experiment conducted on the children in residence. The exact rate of hepatitis infection in children at Willowbrook is unknown; I have seen estimates ranging from 30% to 90% of children becoming infected during their time at Willowbrook. At the time, many specific details of hepatitis were unknown. Willowbrook had a local strain of hepatitis that was reputed to be less lethal than strains common elsewhere. Saul Krugman, funded in part by the U.S. Surgeon General’s Office, began conducting a study on hepatitis in Willowbrook – initially starting with an epidemiological focus, then shifting to a more involved study. Krugman intentionally infected 60 children at Willowbrook with the hepatitis virus by feeding them live samples of the hepatitis virus. Krugman “watched as their skin and eyes turned yellow and their livers grew bigger.”
Willowbrook left the public consciousness almost entirely until 1972, when Geraldo Rivera created a bombshell documentary that exposed the conditions at Willowbrook State School and institutions like it. In March 1972, residents’ parents filed a class-action lawsuit alleging violations of the constitutional rights of Willowbrook residents. Just three years later, as a result of the lawsuit, the Willowbrook Consent Decree created standards the institution would be Willowbrook open, however; Willowbrook State School formally closed “officially and forever” on September 17th, 1987.
Postcard of Willowbrook with a yellow label stating “Willowbrook State School”. Source: New York Public Library Digital Collection
Despite the promise made in the wake of the Willowbrook scandal, alumni are still mistreated today. In 2020, The New York Times published the results of an investigation conducted into recent abuses in a group home in New York where some Willowbrook alumni resided. They describe physical abuse and neglect, including injuries caused by scalding water, deaths caused by neglect, and ant infestations. The investigation made allegations against 13 employees, nine of whom still worked for the agency, and seven of those still worked in group homes at the time of the article’s publishing.
Institutions for People with Disabilities Today
In 2018, the Office of the Inspector General (OIG), along with other federal agencies, published a report on group homes, which have largely succeeded large institutions like Willowbrook or Bryce. They found that, in 49 states, health and safety procedures were not being followed.
“OIG found serious lapses in basic health and safety practices in group homes. OIG made multiple referrals to local law enforcement to address specific incidents of harm.”
Between 2004 and 2010, 1,361 people with disabilities died in Connecticut. 82 of those deaths were caused by neglect or abuse. The causes were found to be due to “abuse, neglect, and medical errors.” The OIG found that “State agencies did not comply with Federal waiver and State requirements for reporting and monitoring critical incidents.” These “critical incidents” include deaths, assaults, suicide attempts, and missing persons.
An older man in a wheelchair being escorted by a caregiver. Source: Yahoo Images
While we, as Americans, often like to think our country has advanced for people with disabilities, the reality is disappointing. Willowbrook alumni are still being abused forty years later. Group homes have been found to have widespread abusive and neglectful practices.
State Protection & Advocacy agencies exist as a legal protection for people with disabilities. In Alabama, the Alabama Disability Advocacy Program provides legal assistance to people with disabilities in cases involving civil rights violations and has the ability to investigate said cases in hospitals, group homes, schools, and any other facilities where abuse or neglect of people with disabilities occurs.
Poverty is a deeply rooted issue that affects countless individuals and communities around the world. In Kenya, it is no different. Despite its natural beauty and richness, Kenya faces significant challenges when it comes to poverty, particularly among vulnerable communities.
The high living standards brought by the new government of Kenya make the poverty issue more pressing. Everything is doubled. Tax is doubled, food is doubled, oil is doubled, women’s products price is now double the initial price.
Masai Market in Kenya; Source: Yahoo Images
One issue arising from poverty is limited access to basic necessities such as food, clean water, and health care. According to a United Nations Development Program report, approximately 36% of Kenyans live below the national poverty line. This means that millions of people struggle to afford even one meal a day, leading to malnutrition and adverse health conditions. Additionally, a lack of access to clean water and proper sanitation facilities further intensifies the spread of diseases, resulting in a higher mortality rate.
The UN World Food Program (WFP) assists many Kenyans who face food insecurity. Source: Yahoo Images
Another consequence of poverty is the limited educational opportunities available to children coming from disadvantaged backgrounds. Before the current government, a normal student at the university level was paying approximately 38 thousand Kenyan Shilling per year. Today the student pays 122 thousand Kenyan Shillings per year. Many families cannot afford to send their children to school due to financial constraints, resulting in a significant number of young individuals being deprived of basic education. The lack of education perpetuates the cycle of poverty, as individuals without the necessary skills and knowledge struggle to find stable employment opportunities.
The impact of poverty is also evident in the housing conditions experienced by vulnerable communities in Kenya. Slums and informal settlements are common in urban areas, where individuals live in makeshift shelters with little to no access to basic amenities. Unsanitary living conditions in these areas increase health risks and disease vulnerability.
A Student with school materials. Nyeri Primary School, Nyeri County, Kenya; Source: Yahoo Images
These challenges are not insurmountable, however. It’s important to note that while these issues persist, there are numerous organizations, both local and international working alongside the government of Kenya to tackle these issues and improve the overall well-being of the Kenyan people. Efforts such as community-based programs, microfinance initiatives, and educational campaigns have shown promising results in uplifting vulnerable communities and breaking the cycle of poverty.
To bring about lasting change, it is crucial for individuals, governments, and organizations to come together and address the root causes of poverty in Kenya. This includes investing in sustainable agriculture practices, promoting entrepreneurship and job creation, improving access to quality education, and providing support for health care and social welfare systems.
Parliament of Kenya; Source: Yahoo Images
In conclusion, poverty remains a critical issue in Kenyan society, affecting vulnerable communities in various aspects of their lives. By understanding the impact of poverty and actively working towards its eradication, we can create a brighter future for all Kenyans.
Even though 1 in 6 people around the world experience disabilities, they are often among the forgotten groups within our society. While people with disabilities today are living under better conditions than their ancestors, there is still a lot of progress needed to be had to ensure that people with disabilities can lead a life of dignity and independence, free from the stigma and failures of society’s ableist mindset. In this two-part blog, we will focus specifically on children with disabilities within the American education system, but before that, it is necessary to frame the historical context surrounding the American education system, and how disability in America has been treated as a whole. As a result, part one of this series will focus on setting the historical context, exploring the American Education System as well as the treatment of people with disabilities throughout American history. The second part of this series will focus on exploring the contemporary issues faced by children with disabilities and their families within the American Education System and learn about a human rights framework for disability rights.
History of America’s Education System
The Unequal Distribution of Knowledge
Image 2 – Source: Yahoo Images
Since the founding of this country is rooted in capitalism, patriarchy, and white supremacy, many groups of people have been historically denied access to education. Traditionally, children from poor backgrounds were expected to help their families on the farm or work in their family businesses to make ends meet. As the industrial revolution took hold, child labor transferred from the farms to the factories, and many industries, such as the textile industry preferred to employ children to exploit their minuscule features. The petite features of the children came into use when they were needed to get into tight spots, or when operating machinery that required smaller extremities. Child labor in America was not outlawed until 1938, meaning that many children from poor families were illiterate and disadvantaged in comparison with children from wealthier families, who could afford to educate their children instead.
In addition to the absence of child labor laws, the patriarchal structure of American society deemed it more important for boys and men to be educated than their female counterparts. While poor families were denied access to education on the whole, even among wealthier families, the education of boys was prioritized over educating women. Women were expected to be homemakers and child-bearers in the private sphere, and the public sphere was reserved for their male counterparts. Many women were denied access to education, were not permitted to participate in politics and were limited to feminine jobs (such as teaching, nursing, and domestic work) when they did participate economically in the larger society. It was not until the 19th century that women were given more flexibility in their pursuit of higher education. Of course, not all women shared the same experiences, and white women were better able to receive education than women from other races, and as expressed earlier, wealthier women had more opportunities to educate themselves than did women living in poverty.
Furthermore, the foundations of white supremacy upon which America was built denied people of color access to education. Education provides the key to empowerment, and the status quo did not want to empower those they deemed to be inferior. Due to the hierarchical nature of this supremacist mindset, people from different groups were “dealt with” in different manners. For immigrants, access to education depended on their country of origin. Some immigrants, such as those from Asian countries, were barred from receiving education in America until the 1880s and were instead used for hard labor, like constructing railroads. European immigrants, on the other hand, were well-received by many in America, (with the exception of the Irish), and were granted many of the rights shared by American citizens at the time. There was however, a difference in treatment between the Old immigrants, (which were members from wealthier backgrounds with skills and education levels from the Southern and Eastern parts of Europe that came to America in the early 1800s), and the New immigrants (who were mostly impoverished, unskilled laborers from Western and Northern Europe who migrated to America in the late 1800s).
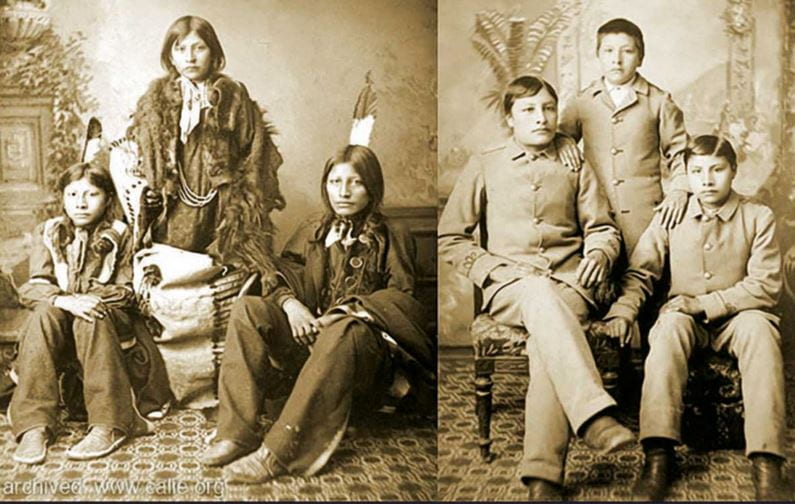
In addition to immigrants, the indigenous population of America also received access to education with a different approach. In an attempt to force them to forget their rich cultural histories and erase the cultural differences between the indigenous population and the larger (White) American society, children from different tribes were kidnapped and forced into boarding schools where they would learn to be assimilated into the American culture. Indigenous children were punished for speaking their language, engaging in their cultural practices, or even wearing cultural clothing (whether it was casually or for cultural practices). This is one of the reasons that today when people appropriate Native American culture (and attire), it can be very insulting, as they were punished for practicing their culture and wearing their traditional clothing.
Image 3 – Source: Yahoo Images;
Furthermore, during the enslavement of African Americans, who were deemed to be on the lowest level on this racial hierarchy, access to literacy was denied to them and outlawed, making it punishable by law for African Americans to be literate. This law was another way in which racist leaders of the time maintained control over the enslaved population. Following this period, there were many racist laws and social barriers to education for African Americans over time, and it was not until the famous passage of the ruling in Brown v. Board of Education that African Americans were given the right to equal education. With all that being said, there is still an ongoing struggle to bring equity, inclusion, and diversity into the American education system.
There can be a whole blog dedicated to the housing market, its impacts on funding for the local schools, and how this influences the level of education the children within those districts experience. As mentioned in previous blogs on similar topics, this funding practice tied to the housing market is, yet another way racism has seeped into American institutions. Transforming the American Education system into a more inclusive one will be a difficult fight ahead, as cries against teachings with an anti-racist approach are molding the current curriculum within the education system today.
The Historical Struggle to Secure the Right to Education for People with Disabilities
Image 4 – Source: Yahoo Images
This exclusive approach to education also historically denied access to disabled individuals as well. American society has been structured with an ableist mindset, and people with disabilities have been stigmatized and marginalized by the larger society. In the past, many states prevented children with disabilities from attending school, choosing to place them in state institutions instead. Some wealthier families with disabled children could afford to home-school them, but the rest of the children with disabilities within society were not given that opportunity.
Even after education was required for all children, many states refused to provide accommodations for their students with disabilities, and the responsibility of securing access and mobility was placed on the children and their families, rather than the state. Judith Heumann, a well-known disability rights activist, was denied entry to her elementary school during the 1950s because the school district deemed her a “fire hazard” for being mobility impaired and having to use a wheelchair. It was not until the passage of the Education for All Handicapped Children Act (EHC; later known as the Individuals with Disabilities Act or IDEA) in 1975 that educational rights were protected for groups in need, including children with disabilities. While education access was protected under this law, the passage of the Americans with Disabilities Act (ADA) in 1990 was needed to ensure that people with disabilities are protected from discrimination in all aspects of society.
The Horrific History of Disability in America
How were People with Disabilities Viewed in the Past, and how has that changed today?
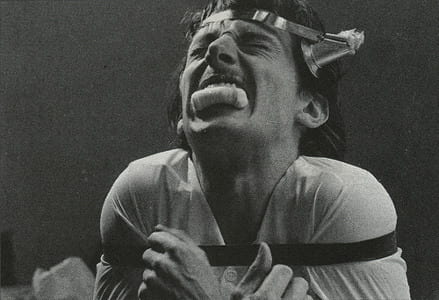
Image 5 – Source: Yahoo Images; An image depicting a man who is audio-visually impaired, being held down as a priest performs an exorcism on him to “free” him from the demons possessing his body. This was a popularly held belief about people with disabilities.
Understanding the historical context behind the American education system is only one part of this conversation. Outlining the lens through which disability is viewed today, and in the past, is necessary to comprehend the treatment of children with disabilities within the American education system. Today, people with disabilities are viewed in four ways. For one, following the traditional views of disability, most people with disabilities are simply ignored by society, both as a population, as well as systemically. You can see this is the case by simply looking at some of the ableist framings of our infrastructure. Needless to say, being an invisible group within society comes with its own challenges.
Another common way society approaches people with disabilities is to view them as the “super-crip” (which is extremely insulting) and look at their achievements as “inspirational.” People who believe this highlight people with disabilities in a supernatural sense, similar to how many African Americans were portrayed as supernatural beings with superhuman strength and abilities. This troupe was not helpful to the African American community then, and it is not helpful to people with disabilities today. Some may argue that this troupe seems to be a positive outlook of the group, but upon closer inspection, it is important to recognize the stress and burden of success this places on people with disabilities to feel accepted by society. It also encourages the mindset that these people who achieve extraordinary things are superhuman and that their achievements are highlighted because there is a general conception that this is abnormal for the group. Additionally, for a person with disabilities, it can be insulting and demeaning to hear the phrase, “if a person with a disability can achieve this, so can you!”
Another tactless way in which people with disabilities are regarded, as inferior to the rest of the population. Many able-bodied individuals either view them as a burden to society or simply objects to be pitied. This can have the impact of treating people with disabilities as second-class citizens and making them feel as if they are lacking in some way or another. Those who show pity toward people with disabilities may have good intentions, but their actions treat people with disabilities as victims of fate, rather than with dignity and humanity.
Finally, some people within society treat people with disabilities as if they have undergone a tragic event (whatever led to their disability), and people require “saving” or “treatment” to be “cured” of their ailments. This too is not the case. People with disabilities adapt to living their lives with their disabilities, and they don’t require anyone to “save” them from their disabilities. This is extremely insulting and rude to even think that, and it has the same connotations as would a “white-savior complex” within the context of race. The underlying belief in both of these situations is that the person doing the “saving” believes that the person that needs to be “saved” cannot do this for themselves and that they require the help of the “savior”.
While it is important to understand the contemporary views of people with disabilities, it is equally relevant to familiarize ourselves with the ways in which people with disabilities have been treated in America in the past. Until the 19th century, people with disabilities were separated from participating with the rest of the larger society. During colonial times in America, people with disabilities were treated in a similar light as the Salem witches, either burned or hanged. Others viewed disability as a sign of God’s disapproval of the colonists, and people with disabilities were treated as though they were possessed. Still, others felt that people with disabilities were a disgrace to their family and their community, and many were shunned from their homes. The larger society lumped criminals, poor people, mentally ill people, and people with disabilities under the same roof, labeling them as outsiders. This practice evolved into the many horror stories that we may be familiar with today regarding asylums and their treatment of their patients. An important note: as it is with other American institutions, racism, and sexism disproportionately impact the lives of people of color and women within these institutions, and this translates into how they are perceived and treated by the larger society as well. This remains true for people with disabilities with identities that are not aligned with the patriarchal, white society.
The mistreatment and abuse of people with disabilities within asylums
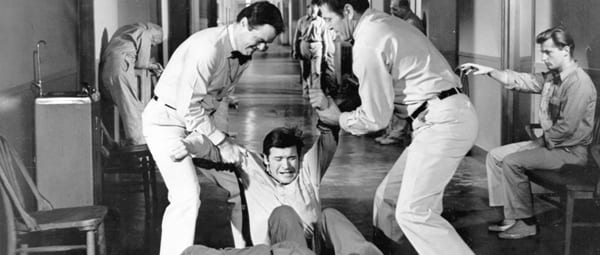
Image 6 – Source: Yahoo Images; An image depicting an asylum, where people with disabilities were forcibly committed. In this image, there is a bed, and a wheelchair in the room big enough for one person, but many facilities were not as fortunately funded or furnished.
People with disabilities, along with other vulnerable groups that were stigmatized by society, were pushed into asylums. These were large “hospitals” stocked with medical equipment and personnel in which the goal was to provide care and treatment for the patients that resided within these asylums. The reason I placed hospitals in quotations is that many of these asylums were simply places to house all the people society did not want. These patients were experimented on, abused, neglected, and had almost no rights to defend themselves. Some patients that were from wealthy families were able to be treated at home, but others that came from meager backgrounds were not as fortunate. Many of the staff working within these institutions were unsympathetic towards their patients, feeling burdened by their very existence. Many people (within the institution and outside in the larger society) believed that people with mental illness and people with disabilities were “acting out” on purpose, to make life harder for those “upstanding” citizens of society. Many of the patients were misdiagnosed, and the institutions went from trying to care for the patients to “cure” the patients of their disabilities. The stigmatization of these groups within the asylums meant that their needs and wants were ignored. In addition to that, because it did not require a professional recommendation from a medical practitioner to admit patients into the asylums, many people were wrongly admitted to these institutions (because of personal grudges or disapproval of their behavior) for years without the right to defend and protect themselves.
Of course, it is not wise to lump every institution together and generalize about their treatment of their patients. While some were genuinely trying to take care of their wards and research ways to help “cure” them, others were less sympathetic to the plights of people with disabilities, both visible and invisible. For one, similar to the issues that American prisons face today, asylums were overcrowded, understaffed, and underfunded. This meant that each individual residing within the institutions was not given the personal care they required, and instead, they were all lumped into groups to receive generalized treatments. This was problematic in so many ways, but the most obvious is that disability takes many shapes and forms, and each individual had different needs that had to be met. Approaching a group of people with disabilities with generalized treatments meant that the doctors and nurses never took time to understand the details of each person’s disability, much less how best to approach them. As a matter of fact, because many believed disabilities to be a spiritual problem (a person being possessed by the devil), early “treatments” for mental illnesses and disabilities came in the form of exorcisms. When medical professionals finally were able to understand that this was a bodily illness, not a spiritual one, they then proceeded to conduct various experiments on the patients without having any knowledge of how to treat their patients. This is where the tortures began.
Image 7 – Source: Yahoo Images
Medical personnel proposed many treatments to “cure” people with disabilities, including inhumane procedures that involved drilling holes into the patient’s skull in an attempt to bleed out the disease in question. While it is easy to judge in retrospect, in the beginning, many of the doctors truly believed that they were “curing” their patients with the various treatments they provided them, even as many recognized the inhumane nature of their treatments.
Other various treatments were administered to the patients, which can be defined as abusive and torturous today. Many women with disabilities were abused sexually, both by other patients and their caregivers. In addition to these incidents, many states (through the support of the law) practiced forced sterilization of disabled individuals in these institutions. The justification for this practice was expressed as cleansing humanity of these various illnesses and disabilities. Inspired by the American practice of eugenics, Nazi Germany expanded upon this practice to include everyone that did not fit their description of the “Aryan” race. To this day, America has not acknowledged this practice, and forced sterilization continues to be legal in the United States because of a Supreme Court ruling in 1927. The case in question, Buck v. Bell maintained that the sterilization of Carrie Buck (a woman who was raped and accused of “feeblemindedness”) was not in violation of the Constitution. This ruling permitted the forced sterilization of thousands of people with disabilities and other traits deemed “unwanted” by the general public. While the Supreme Court has outlawed forced sterilization as a form of punishment, it has never overturned its ruling made in Buck v. Bell. As a result, this practice is technically still supported within the legal framework.
With very little funding, the living conditions within the institutions also proved to be dangerous. The asylum itself was built to be uncomfortable because there was a belief that comfortable living would encourage patients to stay there forever. This meant that there was poor insulation, keeping the buildings cold. Due to the shortage of staff, many patients were restrained or locked up, while others were neglected altogether. These conditions, along with the “treatments” they received, exacerbated the patients’ conditions and were detrimental to their mental and physical health. Finally, as a result of society’s exclusion of this vulnerable population, many people outside of the institutions were not aware of what was taking place within. The patients inside these asylums were all but forgotten, invisible to the rest of society.
Deinstitutionalization
Image 8 – Source: Yahoo Images; When the institutions closed without much warning, many of the patients were left stranded to fend for themselves with no help from the government.
In an attempt to expose these terrible conditions to the larger society, journalists and activists spread accounts about the conditions within the asylums. Many were able to do this by investigating these institutions firsthand, and images (and videos) of the ill-treatment of the patients began circulating. As people started learning about the horrific conditions in which their loved ones were being kept in, the asylums faced a lot of backlashes. Amid all the backlash, in 1946, President Truman passed the National Mental Health Act to begin research on neurological issues. It would not be until 1955, however, that things changed drastically for those suffering from mental illnesses. Thorazine, a psychoactive medication that was introduced as a way to treat mental illness, and the population within the institutions peaked around this time. In the 1960s, there was an attempt to take a community-based approach to treat mental health, but it lacked the funding to progress in any substantial way. In 1981, Ronald Reagan takes a drastic step to stop government funding to help with mental health, forcing institutions to close their doors and leaving the patients on the streets.
This dramatic change provided no cushion for the patients to fall on, and much experienced homelessness as a result. With nowhere to go and no help from the government, many people with disabilities lost their lives because of this policy shift. These individuals never received any compensation for their ill-treatment, nor were they given any transitional housing or aid to help restart their lives. Of those that did not end up dead, many people with disabilities were imprisoned for causing “public disturbances.” Unfortunately, this practice continues to exist today, especially impacting people of color, and people living in poverty disproportionately. Of course, the imprisonment of people suffering from physical and mental disabilities exacerbated their conditions, and the lack of care and treatment resulted in many deaths. With nowhere to go, and no rights to protect this vulnerable population, people with disabilities continued to suffer due to systemic failures.
The movement for disability rights
Image 9 – Source: Yahoo Images;
Eventually, following the lead set by the Civil Rights Movement and many other movements such as the Women’s Rights movement, and the sexual revolution that fought for the rights of the LGBTQ+ community, people with disabilities came together to stand against discrimination toward them from the larger society, and fight for their rights to exist and prosper like any other groups. People with disabilities wanted to challenge the practice of institutionalization and employed many of the tactics that were used during the Civil Rights Movement. They staged sit-ins in governmental buildings like the FBI building, challenged the mobility norms of society by blocking busses (that denied accessibility to people with disabilities) from moving, and they protested on the streets, able-bodied allies and people with disabilities alike, fighting for their rights.
People with disabilities were also exhausted with the ableist society they lived in and began to challenge the many barriers within society that kept them from living as independent individuals. They did not need someone to hold the doors for them; they wanted the doors to remain open automatically long enough for them to pass through. They wanted accessible sidewalks on which they could move their wheelchairs, walkers, and other walking devices (if applied) safely, and independently, without having to depend on others to take care of them. People with disabilities and their caregivers began to challenge the largely held view by society that people with disabilities were a burden to society. They argued that societal barriers made them dependent on others and implementing disability-friendly solutions can provide the community with the independence to live their lives freely.
In 1973, with the passage of the Rehabilitation Act, specifically, Section 504, people with disabilities, for the first time, were protected by law from being discriminated against. This act recognized that the many issues faced by people with disabilities, such as unemployment, transportation, and accessibility issues, were not the fault of the person with the disability, but rather, a result of society’s shortcomings in failing to provide accessible services to the group. While this was a major win for this community, this law only applied to those who accepted federal funding, meaning that the private sector, and even many of the public sector, could still discriminate against people with disabilities. Following the passage of this act, many people with disabilities were instrumental in ensuring its enforcement. Many of the sit-ins referred to above happened at this time, as an attempt to keep governmental offices accountable. Protestors would block the entrances into the government buildings, or stay in the buildings past close time, refusing to leave until the necessary changes were agreed to be made to the buildings (such as including ramps to the building or elevators inside the buildings) to meet the Section 504 requirements. This continued until Ronald Reagan issued a task force to stop the regulatory attempts made by supporters of Section 504, and the protections secured by the IDEA, an act that protected the educational rights of children with disabilities. Over the following years, his decision resulted in hundreds of frustrated parents and people with disabilities alike questioning the justification for stopping the regulatory actions of Section 504. This backlash, accompanied by the tireless leaders of the community meeting with White House officials, ended in Reagan reversing his crackdown on Section 504, allowing regulations to continue on businesses that refused to incorporate practices outlined in Section 504.
Additionally, following the passage of the Fair Housing Act in 1968, people with disabilities, along with other protected groups such as race, gender (and sex), and religion, were protected from discrimination in housing. The first passage of the act initially only included race, religion, national origin, and color, as the protected groups. It was not until 1974 when sex (and gender) were added to this list, and not until 1988 when the disability community was added. Still, this act was especially important for people with disabilities because it required home builders to provide reasonable accommodations necessary for the inhabitants to live comfortably and move around the housing unit.
Following these many small victories came the biggest one of them all, the passage of the Americans with Disabilities Act in 1990 (ADA). This law was the first general law protecting people with disabilities from discrimination in all aspects of society, including in housing, employment, healthcare, transportation, and many other social services that impacted the lives of this protected group. The passage of the ADA focused on four main themes: full participation, equal opportunity, independent living, and economic self-sufficiency. Full participation focuses on the ability of people with disabilities to participate in all aspects of their lives, including having access to transportation, entering and exit buildings without issues, being able to vote on inaccessible sites, and enjoying life without social barriers that prevent them from being able to do so. Equal opportunity centers on being able to be employed without facing discrimination due to their disability and being able to take advantage of other such opportunities free of discrimination. Independent living brings attention to the ableist framework that society is structured in and recognizes the need for a more disability-friendly society, with access to handrails, ramps, curb cuts, and other options such as disability-friendly online sites (that for example, speak the menu out for you if you are a person with visual imparities) to raise the living standards for people with disabilities. The basis of this pillar is to empower people with disabilities with tools they can use for themselves in order to live independent life. Finally, the economic self-sufficiency piece mainly concentrates on the economic security of people with disabilities. This includes access and accommodations to receive higher education, better employment opportunities (including training, transportation access, and mobility within the workspace), and other such necessities to promote economic self-sufficiency within the disability community.
Image 10 – Source: Yahoo Images
Many communities across the United States are brainstorming innovative ways to be more inclusive, but we are far from being a fully inclusive society. People with disabilities remain among the invisible groups within society, not because their advocates are not loud enough, but because their cries are being ignored by lawmakers and their local representatives. Globally, the United Nations established the Convention on the Rights of Persons with Disabilities(CRPD) in 2006, working to shift the mindset of people’s views on disability as a whole, as well as protect and promote the rights of individuals with disabilities by empowering them to fully participate in society with the dignity and humanity they deserve.
While this blog mainly focused on the historical context of the American Education System and the perception of people with disabilities in the past and today, the next blog will focus more on the treatment of children with disabilities within the American education system today, the many challenges they continue to face, how the pandemic has impacted their learning and development, and the human rights framework necessary for disability rights to do what we can to be more inclusive and less ableist as a society.
After decades of systemic and societal discrimination, an array of hope burst through the clouds of despair for transgender individuals. Recently, greater acceptance of transgender individuals in modern culture has opened doors to accessible and evidence-based transgender healthcare. Budding healthcare infrastructure has helped transgender individuals transition and care for their changing bodies providing relief for the marginalized community. Healthcare professionals and teams of scientists worked for decades through societal judgement and the subsequent roadblocks to ensure that the transgender community had an improved chance at a healthy life as non-transgender individuals. However, increasing vitriol exacerbated by politicians has tightened restrictions for gender affirming healthcare across the United States.
Cube beads spelling the word “transgender”; Source: Unsplash
Introduction
In February 2022, Texas Governor Greg Abbott and Attorney General Ken Paxton released a directive stating that gender transition therapies including hormone therapies, puberty blockers, or surgery given to minors can be investigated as child abuse and given criminal penalties. Officials, teachers, parents, nurses, and anyone involved in direct contact with children were required to report suspicions of such therapies, framing the act more as concern for children’s safety and innocence. Anyone found supporting or prescribing such treatment, including parents or healthcare providers, would be subject to child abuse investigations by the Texas Department of Family and Protective Services. The agency was instructed to prioritize cases in which parents who provide their transgender children with gender-affirming care above all other child abuse cases. Strangely, the caseworkers were told to investigate regardless of whether the standard of sufficient evidence was met and to not record their investigation in writing.
Days after the directive was announced, the Texas Department of Protective and Family Services launched an investigation into a federal employee, a mother of a transgender daughter, after she inquired when the directive would be made effective. A federal judge blocked the investigation only 2 days later. In the immediate weeks following the directive‘s release, at least nine families were already facing child abuse investigations for supporting their transgender children in obtaining gender-affirming care. This past spring, the clouds in an otherwise tranquil sky began to blot out blossoming hope as intimidated healthcare providers canceled hormone prescriptions and the few existing transgender youth treatment facilities closed. Families clamored to find alternative sources of hormones and puberty blockers for their children. Some became afraid to claim the transgender label, many moved out of the state, and hundreds more were at home, fighting for their right to exist as their gender identity and as themselves.
Image of protest with posters listing “Transgender Healthcare”
Medical Evidence
In a statement to the Texas Tribune, U.S. Surgeon General stated that this directive interferes with the physician-patient relationship which has no place for religion, beliefs, or politics. Abbott’s directive and Paxton’s following opinion sparked intense backlash from the medical community for blatantly ignoring decades worth of research supporting early transitional care.
When children first learn that they are transgender, they face a physical and mental health disorder known as gender dysphoria. Gender dysphoria is a condition where individuals experience severe dissonance between the gender they identify as and the physical manifestations of their biological gender. Depression, anxiety, and suicidal thoughts often follow this sense of “not self” that plagues many adolescents as they begin to come out to the world with their new name and pronouns. To significantly improve the outcomes of transgender individuals, all major medical organizations including the American Academy of Pediatrics, American College of Physicians, and American Psychiatric Association support gender transition as an effective therapy. Transitioning includes gender-affirming hormonal therapy and puberty blockers. Hormonal therapy begins and allows for a smoother transition into the opposite gender while puberty blockers suppress the body’s natural maturation process to increase the amount of time children and their bodies have to transition into a new gender. In the meantime, individuals receive mental health support and preparation for a successful transition and in unfortunate cases, wait for legislation to increase access to gender affirming treatments.
Overhead view of medications and hormone therapy. Source: Unsplash
The most prevalent medical reason for opposing gender transition is the possibility that a transgender individual will have regrets, because what is done cannot be undone easily. Although it is a valid concern, puberty blockers exist for children and individuals who are uncertain about their gender, because they provide ample time for the individual to choose not to change genders, if that is later realized. In addition, regrets are “extremely rare” and can be attributed to adverse social climates more than personal attitude. Proper mental health support and preparation are also important for a successful gender transition to recognize behavioral changes and tackle the paradoxical shared sentiment that transgender people are no longer welcome in conservative society.
Alabama and Florida Response
Governor Abbott’s attempt to restore conservative values in Texas is not a new phenomenon. Texas has seen several bills criminalizing medical care for transgender children which is reflective of a broader trend across the United States. In the past year alone, 21 states drafted bills to deny transgender medical care. Arkansas passed a bill making it illegal to prescribe puberty blockers and for insurance companies to cover transgender care. Other conservative states, such as Alabama, have taken Abbott’s directive as a green light and are preparing legislation to discourage transgender healthcare and marginalize the LGBTQ+ within their borders. Taking a slightly different approach, Governor DeSantis of Florida introduced what is commonly referred to as the “Don’t Say Gay” Bill (House Bill 1557). Also known as the Florida Parental Rights in Education Act, the bill was signed into law and passed by the Florida Senate in March 2022. This bill would effectively prevent gender identity and sexual orientation education in classroom discussion in Florida. Experts worry that the vague descriptions in the law indicate that it be used it to suppress all actions that remotely fall under the literal definition of sex and gender, leading to a dangerous slippery slope that may open a dark path of minority discrimination.
Black and white image of a protest with the phrase “No Body Is Illegal” centered.
On April 8th 2022, Alabama Governor Kay Ivey signed into law two bills preventing medical professionals from providing gender-affirming care and forcing individuals to use the restroom of their biological gender. In an unprecedented move, the Vulnerable Child Compassion and Protection Act makes arranging gender-affirming treatment including puberty blockers, cross-sex hormones, and surgery for children under 19 a felony with a possible sentence of up to 10 years in prison if convicted. The second bill is culturally similar to Florida’s “Don’t Say Gay” Bill. This bill prohibits teaching or using words related to “sex” and “gender.”
Current Status
A lawsuit filed by families of transgender children weeks after Abbot’s directive was announced resulted in an injunction from federal courts. Abbott vs Doe reached the Supreme Court in May 2022 during which the court ruled that Abbott had no authority to control child welfare officers and direct them to investigate providing transgender healthcare. The country released a sigh of relief, but the fight is not over. Stopping Abbot’s directive seems more akin to a pause on the right’s crusade against the transgender community than a stop.
Recent reports from The Washington Post also suggest that Attorney General Paxton attempted to collect gender marker changes and other transgender identifying information on driver’s licenses from the Texas Department of Public Safety in early 2022. Human Rights Campaign reports that Paxton’s office requested the names and license plates of these individuals later in the inquiry, as well. This news comes as a new shackle for transgender Texans. Some have changed back their gender identity on their licenses to the way it was prior. If not, police or other government officials would know of their transgender identity with the search of their name during traffic stops or unrelated incidents which could lead to dangerous discrimination.
To support the fight for transgender safety in Texas, support politicians and lawmakers who oppose legislation limiting transgender healthcare. Advocate for the reopening of the University of Texas’s youth transgender clinic, the only one of its kind in the southwestern United States, that closed last November. People in Texas and across borders can also donate Lambda Legal and the American Civil Liberties Union (ACLU) which are organizations working to keep the injunction in place on Governor Abbott’s directive after AG Paxton filed an appeal against the federal court decision. They, in conjunction with the Transgender Education Network of Texas and Equality Texas have also assembled the LGBTQIA+ Student Rights Toolkit which is a set of explanations and guidelines to understand Texas’s current plight as well as additional resources such as TX Trans Kids.
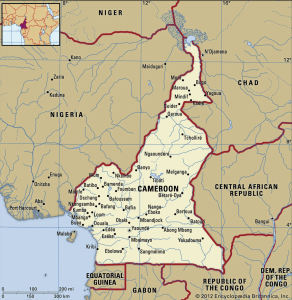
Cameroon, once a bastion of peace and tranquility, is now a nation beset with a series of violent and armed conflicts. Since late 2016, an armed conflict between the state defense forces of Cameroon and the non-state armed groups (NSAGs) of Southern Cameroons’ has ravaged the country. In the last six years, there have been more than 6,000 deaths, 765,000 internally displaced persons (IDPs), and 70,000 registered refugees in neighboring Nigeria, with approximately 2.2 million people in need of humanitarian aid. The Norwegian Refugee Council has referred to the conflict as one of the most neglected in the world. The long-term human capital consequences of this conflict are enormous.
A more comprehensive background of the armed conflict and humanitarian crisis in Southern Cameroons can be found in a previous IHR blog post, “Cameroon, a Nation Divided”.
Source: via Yahoo Images
It is against this backdrop that the Cameroon Humanitarian Relief Initiative (CHRI) in partnership with the Institute of Human Rights (IHR) co-hosted an international webinar, “Updates on the Humanitarian Crisis from the Ongoing Armed Conflict in the Southern Cameroons”on the 18th of October, 2022. The aim of this event was to discuss the current humanitarian crisis from a multi-perspective panel. The speaker biographies can be found at the bottom of this blog post.
Excerpts from this webinar were edited and woven together for this blog post. The full recording of the webinar is available on request by contacting ihr@uab.edu.
Source: via Yahoo Images
Overview
What are the current humanitarian needs for Internally Displaced Persons (IDPs) in Southern Cameroons?
Atim Evenye: The current context and the magnitude of the ongoing crisis in the Northwest and Southwest regions remain tense. There is continuous violence in targeted areas. We have the destruction of properties. We have abductions and kidnappings of both community people and administrators. We have killings and local arrests. We have continuous attacks on schools and students. Humanitarians face threats and direct [armed] attacks. [These are carried out] by both parties, the non-state actors and the state defense forces.
The population [has] really [been] under duress and stress for over six years.
Food Security: Atim Evenye: When it comes to the current needs for IDPs, at the moment, I would say food security remains one of those outstanding needs. Especially in the rural areas, because these IDPs have fled their place of abort. They don’t have access to their farms. [As such,] they don’t have the economic capital [for even] daily subsistence. So, there is a lot of dependencies now on family members, [or] world food programs, and other humanitarian organizations bringing food assistance in the area.
Education Accessibility: Atim Evenye: There is a strict restriction around education. In [the rural areas] of the Northwest and Southwest regions, we have children who have not been able to go to school until date. In urban areas, there is a possibility of schools for those who can afford it. Currently, in our zone in the Northwest and Southwest regions, we have lost one month [of school this term], because we are only starting now. So, it becomes challenging on how to catch up. There’s a need for accelerated learning. [Additionally,] teachers have been abducted [and] schools have been burned. [To add to that,] there is a lot of psychological trauma, [as] many children have witnessed or experienced violence firsthand. Both the state and non-state actors [are] not conscious of the impact their actions are having on children. The government doesn’t want to hear about community schools as prescribed by the separatist. So, it’s really very challenging to access education.
Dr. Emmanuel Nfor: Education is one of the issues at the origin and at the core of the crisis, and formal education has been used by NSAGs, [the non-state armed groups], as a political instrument. NSAGs have advocated and enforced a “no school policy”, leading to public school closures for the past four years in many areas. More than fifty percent of threats against buildings in communities have been directed against schools, and many school buildings have been taken over by organized armed groups. Accessing education in emergency services, or going to school in such a volatile environment, is proven to be risky for children, as well as for teachers. Pupils who were in school in most rural areas have dropped out, some joining armed groups, others displaced, and some have outgrown their ages for the classes in which they were and cannot continue. Many parents have lost their means of livelihood and are unable to sponsor their children in school. Despite repeated calls from humanitarian and human rights organizations for education to be depoliticized, schools have been burnt, teachers and students intimidated, kidnapped, and even killed, and some have seen their hands chopped off by members of armed groups.
Gender-based violence (trigger warning): Atim Evenye: We see [a great deal] of gender-based violence. In certain assessments we have conducted, for example, [many of these] young girls in rural areas are not able to go to school. What are they left to do? There is a lot of harassment, rape, and [sexual assaults]. They’re looking for five hundred francs CFA, that’s like one dollar, to [be able to just buy] food to eat. So then, they depend on young men to give them that money. And at the end of the day, they [get pregnant and become] teenage mothers. The whole cycle is really detrimental, it’s a really difficult one.
Dr. Emmanuel Nfor: Sexual violence is rampant, as a direct consequence of the crisis but also due to decreasing livelihoods, negative coping mechanisms, and lack of protection structures. The boy child is an endangered species, at risk of accusation and arbitrary killing from GFs [state defense forces], and forced recruitment by the NSAGs. There are no specific programs by both UN agencies and Internal bodies that address the needs of the boys.
Housing: Dr. Emmanuel Nfor: If we look at where the IDPs in particular are, we have IDPs that are living in the rural areas, in the bushes. We have those living within host communities. We have some that have been able to rent. [But if] they are able to pay for accommodation, [there are] a lot of difficulties because they want them to pay upfront, and they cannot do it. In all three groups, they lack basic WaSH and health services, NFIs [non-food items], and protection from natural hazards. Those who fled to other regions face stigma and severe protection risks related to exploitation, and socio-economic vulnerabilities including extortion, sexual exploitation, and child labor.
Healthcare: Atim Evenye: The next principal need I would say is around healthcare. In recent times we have [had] heath centers burned, and the staff attacked. So, it’s really challenging. Statement needs to be completed, even before the crisis, access to health care has been a serious challenge, especially in rural areas. And then, currently, with the crisis, it’s even more exacerbated. It becomes difficult now [for] humanitarians on the ground who are trying to meet the needs of these people. Take, for example, Doctors Without Borders. They have [had] to put their activities on the hold because they had issues around access [and safety] of their staff.
Dr. Emmanuel Nfor: [There is a lot of] healthcare [needs] for the vulnerable. [Safe practices in regard to] water, sanitation, and hygiene are not being followed. People who live in rural areas don’t have a good source of water. But they could be educated on the fact that even though your source of water is doubtful, you could take it, you boil it, you purify it, or you do something to make it [potable]. That education, they don’t have, or the chemicals for water treatment. Additionally, there is a lack of emergency medical and psychological units, to provide emergency care to the wounded and psychosocial support to those traumatized by the violence. We can educate people on how to prevent simple infections. How can you prevent diarrhea infection? How can you prevent malaria? If this education is done, it could be [one] way to [improve basic healthcare].
Healthcare, which is supposed to be a protected area, unfortunately, has not been the case in this conflict. We have had health centers closed; more than fifty percent of the health centers in rural communities have been closed. Not only the health centers, [but] the health workers do not feel comfortable staying there. So, a lot of them have abandoned [the centers]. The [people] left in these communities cannot access healthcare. Women cannot access antenatal clinics. Vaccinations [are] not being done, and thousands of children are at risk of contracting common vaccine-preventable infections.
The population has been abandoned to themselves.
Health centers that are open in semi-urban and urban areas are overwhelmed by people who have [been forced by the conflict to flee]. And what’s worse is that most of those who have [fled] do not have the means to pay for the treatment. We have some health centers that have accumulated huge unpaid bills because those who access healthcare cannot afford to pay those bills. For the facilities that are open, IDPs cannot afford to pay for the treatment that is given to them.
We have [also] had cases of drugs and other medical equipment [being] seized along the way by organized armed groups. So, it’s difficult to render care because the drugs and medical supplies do not reach the vulnerable in the hard-to-reach areas. Free supply of drugs and medical equipment is disturbed by locked downs, roadblocks, and/ or are seized at gunpoint.
Then the last very worrying thing is that healthcare workers are being attacked or kidnapped for ransom. A lot of them have been attacked both by the non-state actors and by the state forces; [health workers are] kidnapped by the non-state actors and/or arrested by the [state forces]. So, it is not safe [from] either side. They see you as collaborating with the other, and [so the question is] whether you should treat wounded combatants or not. According to the healthcare regulation, we take any wounded persons as patients. But unfortunately, when these [combatants are] treated, we [the healthcare workers] are blamed. The non-state actors blame you for treating the state forces. The state forces blame you for treating the non-state actors. It’s really a dilemma in which we are in.
Future Directions:
Looking towards the future, are there any resolutions to the humanitarian crisis in Southern Cameroons that you can think of that can be implemented at this point?
Dr. Emmanuel Nfor: I think the first thing we need to consider for the humanitarian crisis is that we need to speak the truth.
We need to make a truthful appraisal of what is happening on the field. Address the needs. For example, we are told that the crisis in Cameroon is one of the least funded in the world. Why? Because the data and the reposting are for some reason concealed.
So, if we must be able to go forward with the humanitarian situation, we need to know how many people are living in the bushes, how many are living in host communities, in what conditions are they living, and be able to address it. [These] figures are often contested, they say the number is lower, or they want to sway the number for their gain. So, we must start with you right data. If we have the right data on needs, it will be possible to see where the solutions should come from.
Possible resolution options, specifically for the humanitarian crisis, could consider the following:
-A community-based approach to raise awareness of protection risks in the community and identify and support community-based solutions.
-Advocate for access to civil documentation, especially birth certificates, to avoid a stateless generation and mitigate protection risks associated with a lack of civil documentation.
-Support community mediation of localized conflicts to reinforce the dialogue between host communities and IDPs and avoid tensions within the communities.
-Advocate with parties to the conflict to respect the protection rights of communities, and respect International Humanitarian Laws.
-Finding durable solutions for IDPs intending to stay in their host communities, like those who have established businesses in the new areas.
-Shelter support in rural areas as a high percentage of households live in tents or informal collective shelters
Atim Evenye: When it comes to setting strategies that we can use to resolve this conflict, I would say it’s imperative, for the powers that be to consider the roles of different parties in the conflict. There is a need for parties in this conflict to come to the table and talk. There is a need for dialogue. There is a need for unity. We need to have a unity of purpose, to push our agenda in one voice.
True is the fact that they have been the major national dialogue, [there] have been consultation meetings and other forms of dialogue in smaller circles. But the question is, during this dialogue are the needs of the different parties considered?
For example, we have women who have suffered a lot as a result of this conflict. But at the same time, we have that arm of women who are also seeking solutions on how to resolve the conflict. Women are now spearheading and speaking for themselves. And I think, there is a need to give a listening ear to what the women are saying because I think time in memorial, women have always demonstrated that ability to resolve conflict. So, one way to consider the proposals that women are giving here in Cameroon.
Secondly, there is a need to give academia and research a place. There are a lot of people in the academic who are gathering data, but the fear around it is the dissemination of this information. The administrative system is such that once you do a publication that is not supportive of what is happening, you get targeted. And by both sides. Thus, we try to be balanced in all information dissemination. There is a need for that deliberation and freedom of speech, especially in the area of academia. People should not be afraid to publicize or to make public the research and the results of what they have found in the field. So that’s another way that can be an added value to the approaches to conflict resolution.
Also, there is a need to consider the root causes. The conflict did not just start like that, it degenerated along the line. So, there is a need to go back to the drawing board and understand what pushed the Southern Cameroonians to arrive at this point. What are the different trends that have been changing through the crisis?
When it comes to how to resolve the humanitarian crisis, I think the humanitarian needs are more than what the humanitarian organizations can do, funding is very limited. It’s obvious that humanitarians cannot meet all the needs. So where should we turn to? We should turn to other actors who can bring assistance. We have development actors who can bring resilient, [long-term, skills-building] projects so that the communities will not be too dependent. The people of the Northwest and Southwest have never been those who are dependent on handouts.
They are people who are hard-working. We hear the aches of people wanting to be self-sustaining. They want to just be, to go back and be what they had been doing [before the conflict].
Dr. Emmanuel Nfor: If we don’t put away falsehood, if we don’t speak the truth and have the right data and have the right information about what is going on, on the ground, we will continue for many more years doing much but with very little impact.
The people of Northwest and Southwest can lead by themselves. These are hard-working people. They just need to be empowered, to go back to where they have lived before. There are many people who are longing to go back home, but the problem is that they go to homes that have been burnt. They go to farms that have been abandoned. They go to be reminded of the horror. So, we need psychological treatment and support. We need some form of equipping them to be able to cope with what they have lost. We should be able to end the hostilities and give people the opportunity to go back home.
So, we should rather empower them, than continue to give them aid. Let peace reign, [so that] we can empower them to reveal what they have lost and then see how they can bring up that life again. [Then] we can go forward. But hostilities should cease, and we should speak the truth; to face each other face-to-face and speak the truth.
Speaker Biographies
Atim Evenye Niger-Thomas, received a Ph.D. in Student Conflict Management and Peacebuilding at the International University of Applied sciences for Development (IUASD) Sao Tome in partnership with IPD Yaoundé. Since 2016, Atim Evenye has worked and grown in different roles at the Authentique Memorial Empowerment Foundation (AMEF). Currently, she holds the position of Assistant Director and trainer for Humanitarian Negotiation. Under this supervision, AMEF has grown to be one of the leading humanitarian organizations in the Southwest Region. AMEF runs four core programs namely,Education and Child Protection (ECP), Economic Development and Livelihood (EDL), Gender, Protection and Peace (GPP), Health/Nutrition/ WASH (HNW).
Dr. Nfor Emmanuel Nfor, holds a PhD in Medical Parasitology from the University of Yaounde I, Cameroon. In February 2017, he joined the Cameroon Baptist Convention Health Services (CBCHS), as the Malaria Focal Point. While working with the CBCHS, he attended a Peer Review Workshop on Humanitarian Negotiation organized by the Centre for Competence in Humanitarian Negotiation (CCHN) Geneva. After many other online courses, and several National and International Conferences, he was appointed Trainer and Advisor of Humanitarian Projects within the CBCHS. In this capacity, he coordinated projects executed by the CBCHS with funding from WHO, UNICEF, and UNFPA. He has been at the forefront of Humanitarian activities within the CBCHS during the ongoing sociopolitical crises in the North West and South West Regions of Cameroon, working closely with the Cameroon Humanitarian Response Plan.
This is the second in a series of blog posts that will look further into the conflict in Cameroon. Each month a humanitarian need and/or organization working in response to the humanitarian crisis will be featured on the UAB Institute for Human Rights’ blog.
Malnutrition in childhood leads to long-term physical and cognitive health effects. By limiting resources to impoverished communities, the DPRK holds control over the bodies and minds of these people. Source: Yahoo! Images
Note from the author: This post is the first of my four-part series on the North Korean Regime. To find the other parts, scroll down and click “View all posts by A. Price.” If the other parts are not available yet, check back in during the upcoming weeks when they will be posted.
Content Warnings: mass financial abuse, famine, malnutrition, dehumanization, classism, starvation
Imagine grocery shopping for your family, and instead of finding a variety of food choices, you find a store filled with a surplus of children’s socks, different colored hats, and beach toys even though you live nowhere near the coast. The only food you can find in the store is a few loaves of moldy bread, a small produce section filled with rotting vegetables, and a frozen section with freezer-burned packaged meat. The best you can do is buy a bag full of rotting vegetables and plant them in the ground behind your house, careful not to be caught doing so by the police. The soil you remember being rich with vitamins has turned to gray dust, and everything you plant dies before sprouting. Your family will live off the rotting leftovers from last week’s grocery trip until you can scrounge together enough scraps to make it through. You know that your neighbor has a secret garden that does moderately well, so you sneak over to offer her what’s left of your money in exchange for a few vegetables. If the police catch you exchanging goods, you and your neighbor will be charged for participating in a free market, thrown in a prison camp without a fair trial, and held for an unregulated amount of time.
The only media you’ve ever seen tells stories of a utopia; the Kim family is sent from heaven to make the Democratic People’s Republic of Korea (DPRK), also known as North Korea, the most wonderful place to live. They tell you that people in other countries, like South Korea and the United States, live under terrible governments who do not care for them the way the Kim family cares for you. In the end, you have no reason not to believe them. You have never seen the conditions of other countries and any criticism of your regime has been consistently disputed throughout your entire life. The stark reality of your consistent mistreatment exists in a dichotomy with the ideals that you have been brainwashed to believe to be true.
Approximately 20 million rural North Koreans live in this reality…
Songbun
The class system of North Korea is called Songbun. At birth, each North Korean citizen is labeled as core, wavering, or hostile based on their place of birth, status, and the national origin of their ancestors. For example, a person whose ancestors immigrated from South to North Korea will be given a low Songbun and be assumed to have genetically inherited hostility towards the government. One’s Songbun can never be changed, as it determines every aspect of one’s life including how resources will be allocated to your community and how much mobility you will have throughout the state.
The Hierarchy of the DPRK. Source: Diagram made by author.
The Command Economy
The Workers Party of Korea (WPK), more commonly known as the North Korean Regime, holds tight control over the command economy and uses it to abuse all people of low Songbun, specifically those who live outside the capital, Pyongyang. Instead of ordering the production of valuable goods like food and home maintenance products for their communities, they overproduce menial things, like children’s socks and beach toys. Many do not have the mobility to go to a neighboring town for resources, and as I will expand on later, many believe that they deserve to starve if they are not entirely self-sufficient.
This economic system has the dual effect of limiting opportunities to participate in the job market. People are not allowed to sell products unless they are commanded to do so by the WPK. Because the WPK is not tasked to create job opportunities for rural people, these people have no opportunity to make money, which only exacerbates the problem of reduced resources.
The overproduction of menial things at the expense of food and necessities. Source: Yahoo! Images
The March of Suffering
The culture that encourages the idea of “suffering for the greater good” is called juche. Juche is the Korean term for the culture of self-sufficiency. It is an idea that is pushed hard into the minds of all North Koreans. Asking for help, depending on friends or family, or participating in a small-scale economy of goods with your neighbors makes you an inherently weak person because you are expected to work harder instead of “begging”. This idea is so ingrained in the minds of North Koreans that they will accept immense abuse from higher-ups at the expense of asking for help or demanding rights.
Starting in 1990, a great famine swept the nation under the rule of Kim Il-Sung. He coined the term “The March of Suffering” to refer to the famine. Using this name, he convinced those who took the hardest hit, the rural people of low Songbun, that they were doing the most honorable thing for their country by suffering in this famine. They were dying for it. Kim Il-Sung glorified their suffering by convincing them that not only did they deserve it (juche), but that their suffering was contributing to the greater good of the country. He had such control over the minds of these people that they loyally followed him straight to their graves.
Handled correctly, this famine could have lasted no longer than a year, and would not have become nearly as severe as it has. Instead, estimates from Crossing Borders suggest that between 240,000 and 3.5 million people have died in the DPRK from malnutrition since 1990.* The famine has outlived not only Kim Il-Sung but also his predecessor Kim Jong-Il.
*The reason for such a wide range of statistics is that collecting accurate data in North Korea is virtually impossible. I expand on the use of outside media control in the second part of this series titled, “How the North Korean Regime Uses Cult-Like Tactics to Maintain Power.”
Even in Pyongyang, vibrant colors are rare. The buildings are drab and dull, the trees are dead, and people dress monochromatically and uniformly. The person in bright blue serves as a traffic director. Source: Flickr
Suppose the topic of North Korea is interesting to you and you want to work towards clearing up the fog surrounding the nation. In that case, I highly recommend Dying for Rights: Putting North Korea’s Human Rights Abuses on the Record by Sandra Fahy. This book is very informative and one of the only easily accessible, comprehensive accounts of North Korean human rights. It is where I learned most of what I know about the DPRK. It set the baseline on which I built my entire comprehensive understanding of the social systems at play.
The cover of the aforementioned book. Source: Fahy, Sandra. Dying for Rights: Putting North Korea’s Human Rights Abuses on the Record. Columbia University Press, 2019. Picture taken by A. Price.
As I will expand upon in the rest of this series, it is imperative that people outside of the DPRK “clear the fog” and find ways to look into the state. One of the biggest motivators for activism is awareness. As people on the outside, some of the most valuable things we can do are spread awareness, garner activism, and bring that activism with us into our participation in the government, whether that be running for office or simply voting for people who share our concerns.
UAB is an Equal Employment/Equal Educational Opportunity Institution dedicated to providing equal opportunities and equal access to all individuals regardless of race, color, religion, ethnic or national origin, sex (including pregnancy), genetic information, age, disability, religion, sexual orientation, gender identity, gender expression, and veteran’s status. As required by Title IX, UAB prohibits sex discrimination in any education program or activity that it operates. Individuals may report concerns or questions to UAB’s Assistant Vice President and Senior Title IX Coordinator. The Title IX notice of nondiscrimination is located at uab.edu/titleix.