In retaliation to a day celebrating the world’s best-known colonizer, the infamous Christopher Columbus, on October 11th, Indigenous People’s Day highlights the culture, struggles, and history of America’s indigenous population. A silent struggle, however, persists: disease.
Native Health Disparities in COVID
The early 1600s brought to America the infamous two Gs—guns and germs—the latter proving the most deadly as bouts of influenza took a toll on Native American populations across what is now the United States. In the age of modern medicine, it comes as a surprise that disease still wreaks havoc on America’s indigenous population. The ongoing COVID-19 pandemic is no exception.
This vast gap is a reflection of poor medical and public health services for Native Americans. Health disparities that plague the Native population include diabetes, heart disease, and rates of addiction to harmful substances. These follow a similar pattern of COVID-19 with Natives being more likely to experience these chronic conditions compared to all other racial categories. These disparities could potentially be alleviated by greater equity in access to medical and public health services, but a fundamental issue in providing this care lies in Native sovereignty. As determined by Worcester v. Georgia, 31 U.S. 515, Native American land, or reservations, are considered sovereign land. While at face value this seems to be a win empowering Natives and acknowledging their right to the land that was once theirs, it creates a vacuum of public services.
Encapsulated by possessors of what was once their land, Native health and well-being are bound by the constraints of the state. A lack of widespread taxes, natural resources, and human resources leaves the reservations reliant upon the ‘external’ state of America for support and sustenance. Most money generated on reservations largely consists of gambling and casino money—practices usually outlawed in the surrounding states. This money only goes so far in providing for the tribe as money often stays within certain families, leaving the rest of the reservation in high rates of poverty. Thus, the main provider of health care for nearly 2.2 million members of the tribal communities, the Indian Health Service, is funded by American tax dollars. And yet, the IHS’s hospital system is severely underfunded and understaffed. The main mechanism created to fight disease seems designed to fail. In this sense, disease continues to persist as a remnant of colonialism, which directly violates the fundamental human rights to accessible health care and to acceptable standards of living.
Unsplash
Vaccination Rates on the Reservation
The only light at the end of the tunnel is the rapid rate of Native American vaccination against COVID-19. While co-morbidities and co-mortalities make it such that if COVID is contracted, Natives will be more susceptible to death, the COVID-19 vaccine acts as an equalizer. Once vaccinated, the likelihood of death by COVID-19 significantly decreases.
Native American tribes have been able to boast proud levels of herd immunity with large tribes like the Navajo Nation at roughly 70% fully vaccinated as of May 2021. This commendable statistic is a result of rallied community effort. Cultural values of supporting the elderly and a strong sense of family and allegiance to the tribe—values typically highlighted in Indigenous People’s Day—worked in favor of creating a climate in strong support of vaccination and vaccine acquisition.
Unsplash
Looking Ahead
While the tide has turned in favor of Native Americans, preventing them from being labelled as another health disparity statistic in COVID-19, it is important to remember and to look towards long-term health care equity and solutions for Natives. While increasing funding for the IHS is certainly a good starting point, robust public health interventions and funding for community programs is necessary. Funding dollars from the top could in theory trickle down, but grassroot rallying and support for public health interventions in a community where cultural values of togetherness and unity already exist could prove to be the needed impetus for transforming not only health care access and quality for the Native American population but also general standard of living that leads to health baselines which are robust to disease.
My most recent article described an overview of the opioid addiction crisis from a human rights perspective. You can view it here. In this article, I attempt to explain the different solutions from medical professionals regarding opioid addiction and the racial and economic disparities that have arisen amongst the most successful solution.
There are two forms of treatment that most clinics can decide between: traditional counseling therapy with a focus on mental strength or using medication, such as buprenorphine and methadone, to combat addiction. Research has proven that without medication, people are twice as likely to die from an overdose. However, the traditional counseling methods have persisted across treatment centers. The Journal of Substance Abuse conducted a study that showed that between 2003 and 2010, of 50,000 opioid addiction patients on Medicaid, patients who had received counseling therapies were six times more likely to relapse than those who received methadone as treatment and four times more likely than those who received buprenorphine. The risk of overdoses is increased during the period of detoxification utilized by abstinence based programs because of a lack of tolerance.
Counseling. Source: Alan Cleaver. Creative Commons.
Opioid substitution has proven to reduce mortality. To avoid a misuse of buprenorphine and methadone, the two medications are tightly controlled by doctors. Buprenorphine is a drug that reduces the craving for opioids and reduces the chances of a fatal overdose overall. Suboxone, a compound of buprenorphine, is engineered to reduce the possibility of an overdose. However, using medication as treatment for addiction has only truly been utilized at a small number of walk-in clinics and has not been fully incorporated into the nation-wide health care system. In 2015, in the United States, 8-10% of treatment programs offered buprenorphine and methadone as substitution therapy. Even in this small number of programs, the method was often unsuccessful as the medicine was offered for too short of a period to be effective. The treatment is only provided in very regulated clinics and prescribers are limited to a maximum of 275 patients.
Between 2012 and 2015, the number of doctor visits where the health professional prescribed buprenorphine greatly rose. Despite this, a research report found that of 13.4 million medical cases involving buprenorphine, there was no increase in prescriptions written for minority groups. Dr. Pooja Lagisetty, one of the authors of the study, reported that white populations are nearly 35 times more likely to have buprenorphine discussed in their visit than black populations. Accessibility and insurance ability are commonly cited as reasons why this disparity has occurred, especially as the majority of white patients paid for their treatment using cash or insurance whereas only 25% of visits were covered by Medicare or Medicaid. This is especially concerning when it is taken into consideration that the rise in the use of buprenorphine occurred at the same time that opioid overdose related deaths were rising significantly faster for black populations than for whites.
The cost of healthcare. Source: ImagesMoney. Creative Commons.
In many cities, opioid addiction treatment is segregated by income. Lower income patients find themselves needing to attend a clinic in order to receive treatment while more affluent patients are able to avoid the clinic and instead receive treatment from a doctor’s office where medicines can be prescribed. These clinic programs are federally funded and often covered by Medicaid. However, in order to receive treatment from the highly regulated clinics, patients must visit daily. Many patients commute for hours every day before waiting within the clinic to receive their life-saving medication. These patients, who are already part of a lower income bracket, are losing precious hours where they could be working or with their families. Work, childcare, families, and other related life events must revolve around the daily trip to the clinic. Some patients have described needing to turn down job offers. Because of this, methadone has earned the nickname, “liquid handcuffs.”
In order to prescribe buprenorphine, physicians are required to undergo a special form of training. Only 5% of physicians have participated in this training. The shortage of clinicians has resulted in the ability of physicians to demand cash payments in return for a prescription of buprenorphine. 40% of white patients paid cash while 35% relied on private insurance. Just 25% of these visits were covered and paid for by Medicaid and Medicare. These percentages highlight just how costly a lifesaving prescription can be for people of low income. Because of the racial disparities within the United States economy, the people who fall into this category tend to be of a minority group. Gentrification has also caused a problem within the clinic community as their buildings get bought out in favor of other businesses. In 2016 in New York City, 53% of participants in methadone programs were Latino and 23% were black, while 21% were white. Also, in 2016 more than 13,600 people in New York filled at least one prescription for Suboxone with nearly 80% of these 13,600 paid for the medication using private insurance.
No More Drug War. Source: Neon Tommy. Creative Commons.
Buprenorphine was purposely introduced into a private market, intended only for those who could pay a high price. Therefore, the unequal distribution of the drug can be determined to be not accidental. Due to the government regulations surrounding the prescription of the drug and the training required for doctors, there are too few doctors actually allowed to prescribe the medication. Those who can often do not accept insurance for their services as demand is so high and they can make more of a profit. Insurance will pay for the actual drug, but patients must pay for the doctor out of pocket.
A permanent stigma surrounding methadone has developed, hailing from the War on Drugs days in the 1960s. Racially charged stereotypes regarding addiction have fueled this stigma which has in turn caused lawmakers to be reluctant in passing legislation that would make the drug more accessible to underprivileged populations. However, this would be the push the community desperately needs. Medicines like buprenorphine and methadone need to be significantly more accessible, both for patients and doctors alike. They need to be included in more clinics while therapy based solely on mental counseling should be phased out from the common addiction treatment centers. In order to close the racial and economic disparities within this crisis, it is important to first recognize them. Once that has been done, our communities need to take direct action that will result in a positive change.
Ubiquity of the novel coronavirus (COVID-19) has drastically changed the way we behave in almost every corner of life. One silver lining drawn into these unprecedented times is that many people are more appreciative of their families, friends, and communities. However, the odds of being in a social network that knows someone who has been diagnosed or died from COVID-19 are greater if you are a racial/ethnic minority living in the U.S. As such, this blog focuses on COVID-19’s disproportionate effect on communities of color and how a human rights approach can help address racial/ethnic health disparities.
Not only do Black Americans disproportionately live in many of the U.S.’s early COVID-19 hotspots (e.g., Detroit, New Orleans, and New York), they are also more likely than their White counterparts to experience poverty and have no health insurance. For centuries, the labor of Black Americans has been deemed “essential”, while the COVID-19 pandemic adds insult to injury. In the medical field, Blacks are less likely to be health professionals and more likely to represent personnel that cleans, provides food, or work in inventory. As such, Black essential workers who are not on the frontlines are more likely to acquire COVID-19 in the pernicious form of regularly contacting cardboard, clothing, or stainless steel. Thus, health disparities in the Black community demonstrate how the legacy of slavery and segregation thrive in the social and economic conditions of COVID-19.
A recent Pew poll found that Latinos are almost 50% more likely than the average American to have been laid off or lost a job due to the pandemic. This is particularly salient to Latinos with a high school education or less and those ages 18-29. However, immigrant Latinos were less likely to lose their jobs but more likely to take a pay cut. As a result, the Latino experience during the COVID-19 pandemic is not only fraught with social and economic drawbacks, much like other communities of color, but complicated by the fact that their large immigrant population is ineligible for needed resources and often relied on in the essential workforce. These outcomes suggest the social and economic consequences of COVID-19 are uniquely challenging to Latinos, namely immigrants with limited access to resources that are often afforded to citizens.
Overlooked: Native American, Native Hawaiian, and Pacific Islander Health Disparities
Thank you essential workers! Source: spurekar, Creative Commons
Health and Human Rights
Health is argued to be a fundamental human right. Ways this can be achieved is through creating greater access to safe drinking water, functioning sanitation, nutritious foods, adequate housing, and safe conditions in the workplace and schools. As such, health exists well outside the confines of the typical health care setting. However, the U.S. has yet to officially ratify the Universal Declaration of Human Rights which ultimately prevents the government from being held accountable for the socioecological influences that generate health disparities across racial/ethnic minority groups.
Despite these discrepancies, the COVID-19 pandemic serves as an opportunity for social change. More specifically, these unprecedented events bring greater light to issues such as poverty, homelessness, unemployment, and migration, all of which disproportionately affect communities of color. As a result, the ubiquity of COVID-19 has gathered people from every corner of the justice community to declare that health is a human right, thus bringing us one step closer to true equity and inclusion.
How to make most of doctor’s appointment. Source: Army Medicine, Creative Commons.
COVID-19 has had a significant impact on the lives of billions across the globe from a disruption of our daily lives to the loss of loved ones to the severe financial burden that has been placed on the world economy. One aspect of society that has been disproportionately affected is the healthcare system. Aside from the financial impact on healthcare systems the way we receive our general healthcare is changing rapidly with this new pandemic. While our primary concern internationally is getting control of this pandemic, non-infectious and chronic conditions are still prevalent and at an increased risk of being neglected.
With the increase in COVID-19 cases in every part of the country, people are being discouraged from coming to hospitals and doctors for non-emergent care. This means that primary healthcare visits either have to be postponed or done through telehealth, which is a remote visit. While telehealth is a great way to have normal checkups without having to go to a doctor’s office, many insurance plans don’t cover telehealth, which makes it harder to afford necessary visits safely.
Additionally, many people no longer have the financial stability they used to. With the downturn in the economy, not only are people who are working making less, but there are also some that have been laid off or furloughed and no longer have access to insurance through their employer. A quarter of those that remain insured have deductibles that are $2000 or higher, which they can no longer afford. This means that in addition to postponing primary care visits, more emergent and necessary visits are being put off.
Those with chronic conditions face more barriers than before to receiving health care. Those with underlying conditions are more likely to have a severe case if they contract COVID-19. However, they need continual care that must be done at least occasionally face-to-face. For example, people with cancer must continue to receive treatment, but many times that treatment makes them immunocompromised. Because of the increased risk, many hospitals no longer allow visitors in, which can decrease patient morale. Many patients also run the risk of having their treatment delayed due to coming in contact with someone that has tested positive for Covid-19. Many chronic conditions, like cancer, are time sensitive, so delays in treatment can be devastating.
Another group of people that have had their healthcare greatly impacted by COVID-19 is pregnant women. There are many check-ups that women are recommended to attend when expecting a baby to ensure the best health possible. However, with the pandemic, that has become harder. There is no evidence that pregnancy makes it more likely to have a severe case of COVID-19. Additionally, there is no evidence that it can be transmitted to a fetus. It’s still important that pregnant women do everything they can to prevent coming in contact with COVID-19. To help in that effort, many OB/GYNs have reduced the number of visits pregnant women should attend in person, switching these visits to telehealth visits.
While a mother cannot pass COVID-19 to her unborn baby, the baby can contract it after birth from her or any other caregivers. To prevent spread to new babies, nurses, and doctors, many mothers are tested when they arrive at the hospital to give birth. Additionally, those that have scheduled C-sections are sometimes tested at home.
Dusti Tellez, a registered nurse at Naval Hospital (NH) Jacksonville’s maternal infant unit, holds a newborn baby for a checkup. Source: U.S. Navy, Creative Commons
According to UNICEF, around 116 million babies will be born during the COVID-19 pandemic. These babies along with the babies born shortly before the pandemic will be missing important doctor’s appointments. The appointments in the first two years of a child’s life play a large role in the child’s overall health for two reasons. First, children will typically receive vaccinations at these appointments, which will keep them from contracting deadly, but preventable diseases. The growing number of children who will not be receiving their vaccinations on time raises concerns about outbreaks of diseases that we’ve kept at bay while also still in the midst of the COVID-19 pandemic. Second, these visits are a good way to track the health of children early as screening for conditions, such as developmental delays, are frequent, and catching them early can give kids with these conditions a helpful jumpstart. Because of these two reasons, many experts advise parents to keep children’s visits up to date, but parents are still hesitant.
In addition to regular checkup visits, people are hesitant to go to the emergency room when they need to for non-COVID-19 related illnesses and emergencies. Hospital visits in the Baptist Hospital system in Memphis, TN were down 27 percent between March 15 and April 15 compared to the month before. Additionally, they noticed that the people that were coming in were more likely to have to be admitted instead of treated and sent home. This means sick people are staying at home longer for fear of COVID-19, and some are dying at home from treatable conditions.
Finally, there are areas of healthcare that are overlooked when we mention essential healthcare workers. My mother is a home health physical therapist, which means she goes to people’s homes to work with them. She mainly works with elderly people, and often visits nursing homes and assisted living facilities. According to her, these places have stricter requirements than before when it comes to letting people in: visitors have to have their temperature checked and have a symptom screening. Some facilities don’t even allow visitors anymore, even for wound care or physical therapy. While therapy might not seem essential, it is often used in this population to prevent accidents, like falls, that would send them to a hospital, where they would be even more at risk of contracting COVID-19.
While many of the changes to the healthcare system are temporary, like the decrease in general healthcare visits, some may become permanent. Telehealth has been shown to be beneficial for healthcare visits that don’t require tests and scans. In fact, many shy children have felt more comfortable with these visits. Additionally, the precautions taken by nursing homes and assisted living facilities when it comes to screening visitors make sense during flu season as the flu kills the over 65 population at a disproportionate rate. While the pandemic has changed some things for the worst, it has also helped us find where some changes need to be made to increase our safety in the future.
Access to healthcare is one of the biggest predictors of health. When someone has access to healthcare, they are more likely to seek treatment for and catch chronic diseases in early stages. This can greatly improve health outcomes and quality of life. However, when access to healthcare is restricted in any way, health outcomes and quality of life decrease, those who need consistent treatment may go without, and preventable deaths increase. Rural areas disproportionately face decreased access to healthcare, which greatly affects the health and productivity of these already disadvantaged areas.
Lack of Insurance
There are many barriers to healthcare that rural Americans face. First of all, there is a lack of insurance. This is mainly because insurance premiums are more expensive in rural areas than they are in urban areas. Urban areas have larger populations, which encourages more insurance companies to compete with each other, driving the costs of premiums down. Additionally, their larger population means the cost of medical expenses can be spread among more people. This also lowers premium prices. Because these two factors are not present in rural areas, they are left without affordable healthcare.
Additionally, many people in rural areas have incomes that fall in the gap between qualifying for Medicare and being able to afford private insurance. Medicare is available to specific low-income groups. In states that haven’t expanded Medicaid, the most common income limit for Medicaid eligibility is 43 percent of the Federal Poverty Line and childless adults are excluded regardless of income. These qualifications leave over 2 million adults in the United States uninsured. Insurance is important because it can help cover costs of healthcare which can otherwise become insurmountable. Those without insurance are less likely to seek healthcare, and when they do, it is typically worse quality than those with insurance receive. Additionally, when an uninsured individual does seek healthcare, the costs are sometimes too high and turn into medical debt. Since much of the rural population is uninsured, these problems plague many of them.
Closing Hospitals and Pharmacies
Those that do have insurance still face a bigger problem: many rural areas don’t have hospitals within a twenty-minute drive. 25 percent of those living in rural areas report that they have to drive at least 30 minutes to get to the nearest hospital. In fact, almost one in four rural Americans say access to adequate healthcare is a major issue for them. Additionally, many hospitals in rural areas are shutting down, leaving communities without the healthcare they are used to. Since 2010, there have been over eighty rural hospital closures, mainly in the southeast. These hospital closings have a devastating effect on the communities they were a part of. Mortality rates for accidents, heart attacks, strokes, and anaphylactic shock risedue to longer ambulance rides. Additionally, residents may be unable to attend routine appointments because of transportation limitations; much of the rural population is elderly, which restricts their ability to drive, and public transportation is less common in rural areas than urban areas. This also means that with the onset of troubling symptoms, residents of rural areas may wait longer to see a doctor because of the inconvenience.
Many rural areas also lack pharmacies, which can hurt those who rely on prescription drugs for good health. Even the rural communities that have hospitals may lack a pharmacist, and many of the pharmacies in rural areas are in danger of closing; many have already. This is due to higher costs of medications at rural pharmacies and lack of pharmacists in rural areas. This can have a devastating effect on residents, as many go periods of time without their prescriptions—like Insulin or medication for depression— until they can get to the nearest pharmacy. Additionally, pharmacists in rural areas are helpful in educating the community on when they can use over-the-counter meds and when patients should see a doctor.
But why are hospitals and pharmacies closing? They have few patients, many uninsured, and they are greatly affected by states’ refusal to expand Medicaid. Medicaid expansion, which 14 states have not ratified, would close the gap between those that qualify for Medicaid and those that can pay for private insurance. As discussed previously, those with insurance are more likely to seek medical care, which would bring more business—and therefore, funding—to hospitals and pharmacies, making them less likely to close. Additionally, they lack the staff required to stay open. 99 percent of students in their last year of medical school report they plan to live in communities with over 10,000 residents. Without a staff, a hospital cannot stay open.
Lack of Specialists
In many rural areas, including those with hospitals, there’s a lack of specialists, like oncologists and OB/GYNs among others. Specialists typically work in large hospitals that have adequate resources, so they tend to reside in cities. This means that those with specialized needs often have to drive to the nearest city to receive care. Traveling can pose a problem to many rural Americans as many of them are older, but this also affects many younger rural inhabitants as they may not have the time off from their jobs to drive hours to receive specialized care. This leaves many without treatment that they need and worsens health outcomes. This is especially concerning considering many rural communities have higher rates of diseases than urban communities do. Specifically, “rural African Americans have higher rates of cancer morbidity and mortality than other rural residents and have higher rates of comorbid conditions” according to Robin Warshaw from the Association of American Medical Colleges. Rural African Americans also have higher rates of disease than urban African Americans. This makes the fact that specialists are not easy to access even more concerning, especially considering they are the largest rural minority. Minorities in general have less access to healthcare, and living in an area that doesn’t have easy access to healthcare in general can exacerbate this issue.
Low Health Literacy
The healthcare system is complex, which means that patients have to work to understand what care they need and when they need it. The ability to do so is called health literacy. Studies have shown that health literacy is important to health outcomes. The higher level of health literacy a person has, the more likely they are to seek out preventative care, such as screening tests and immunizations, that can catch diseases in early stages or prevent them altogether. If a patient doesn’t understand what the doctor tells them, they are less likely to be comfortable enough to seek care. Additionally, higher health literacy rates make it easier to understand how to manage existing conditions. In addition to less access to healthcare, rural Americans have lower health literacy, which compounds their health problems. However, because rural citizens are less likely to have access to health care, it is especially important for them to have high health literacy, which can be attained by using programs that work to educate patients and clinicians on the importance of patients having an active role in their healthcare.
Solutions
Rural healthcare in America is a big problem, but it can improve. In addition to the health literacy programs, there are many solutions to close the gap in healthcare between rural and urban areas. While the common medical school experience trains students for work in populated areas, a consortium of 32 medical schools has created a rural healthcare track with their medical schools. This not only puts more doctors in rural areas, but also trains them for rural areas’ specific health needs. While the program is too new to see a significant increase in rural healthcare professionals, the majority of students who have gone to residency have stayed in rural areas and are studying specialties that are in much needed in rural areas. Additionally, there are many scholarships for those planning on practicing medicine in rural areas, further encouraging medical students to practice in areas in need of doctors.
ELEICOES 2013 NA VENEZUELA. Source: Joka Madruga, Creative Commons
The current president of Venezuela, Nicolás Maduro, was elected in 2013 by a very small margin. During his first term, the Venezuelan economy took a turn for the worst. He was reelected for a second term in 2018, but his opponents feel that the election wasn’t valid because many of the other candidates were made ineligible to run or even jailed, so the National Assembly does not recognize his presidency and considers the presidency vacant. According to the Venezuelan Constitution, in cases of a vacant presidency, the leader of the National Assembly (currently Juan Guaidó) takes over as president. Guaidó has very little political power because the military still supports Maduro.
I first heard about the political and economic unrest in Venezuela when I went on an exchange trip to Spain in May of 2016. My host family had moved to Spain eight months earlier because their jobs had been the first affected by the economic downturn. They were lucky that the dad was a Spanish citizen—it was much easier for them to move to Spain than if none of them had been citizens—but many Venezuelans have not been so lucky.
Venezuelan Protests. Source: Trong Khiem Nguyen, Creative Commons
Since 2015, health statistics have been underreported—if they’ve been reported at all. December of 2016 marked the last report from the Venezuelan Ministry of Health. This report describes an alarming increase in previously eliminated and controlled infectious diseases, such as malaria and diphtheria, and in maternal and infant mortality rates. The report has many alarming statistics, but aside from that, it is the last one to have been published. Additionally, the Health Minister who published the report was fired immediately afterward.
With no one within the country reporting on the health needs and statistics of the people, it is nearly impossible for other countries to give external aid. Additionally, even when aid sent, the Venezuelan government refuses help. Even nongovernmental organizations (NGOs) are forced by law to refuse help: the Supreme Court ruled in 2010 that any NGOs receiving financial assistance from other countries would be committing treason. This has a devastating impact on the citizens as they are not receiving the help that they need.
The situations in the hospitals are dismal. According to a survey conducted by the political opposition, many services in hospitals are not consistently available, if at all, due to lack of supplies. Many supplies have gone missing from public hospitals and clinics, and those being shipped in often are embargoed and never make it past the ports. The reason is unknown, but many suspect it has to do with the corruption of the government. This has forced patients to bring their own medical equipment—which can include anything from medicine to surgical equipment—when going to the hospital, so they know they’ll have what they need. Private clinics, which have most of the supplies they need, ask for payment in US dollars, which means only the wealthiest can get that level of care. This leaves the average citizen without proper medical care in a country where the government is actively keeping lifesaving materials out of the hands of doctors.
Because of the low levels of health care, many diseases are reemerging and worsening. Between 2008 and 2015, there were no cases of diphtheria reported and one case of measles reported. However, in the past three years, over one thousand cases of diphtheria and over six thousand cases of measles have been confirmed. These statistics show a lack of vaccinations in children, which is potentially due to limited vaccines available. Malaria rates, which were once controlled through pesticides, medication, and reduction of mosquito breeding areas, have increased by over ten times from 2009 to 2017. Tuberculosis cases more than doubled from 2014 to 2017, which is even more concerning with the cases of untreated HIV on the rise as well. According to the Human Rights Watch, “Venezuela is the only country in the world where large numbers of individuals living with HIV have been forced to discontinue their treatment as a result of the lack of availability of antiretroviral (ARV) medicines.” 90 percent of HIV positive Venezuelans have to live without ARV medicines, and these people are majorly susceptible to and will be severely affected by the many diseases that are on the rise. Because all of these diseases are on the rise and the limitations of hospitals, maternal and infant mortality rates in Venezuela have risen back to their levels from the 1990s. Venezuela is the only Latin American country where this has occurred.
In addition to the health crisis, there is also a nutrition crisis. The last nutrition data published was in 2007, but many Venezuelans report only eating yuca or a tin of sardines for their one meal of the day. According to the UN’s Food and Agriculture Organization (FAO), 11.7 percent of the population is undernourished, meaning they are not getting enough nutrients. This is severely affecting Venezuelan children; as of March 2018, 17 percent of children under 5 in lower income areas of Venezuela have moderate acute malnutrition (MAM) or severe acute malnutrition (SAM)—a 7 percent increase from February 2017 and a level of crisis. According to WHO, the fatality rates for children under the age of five who have SAM and MAM are between 30-50 percent, so it is important that children not only have access to healthy food, but that hospitals also have access to the necessary treatments, and at this time that is not generally the case in Venezuela. Pregnant women are also affected by MAM and SAM, which can lead to adverse outcomes during pregnancy, childbirth, and the child’s infancy.
Venezuela is not the only country that is experiencing a health and food crisis. However, many countries have these issues due to lack of resources, funding, or aid. While Venezuela is experiencing an economic downturn, they have been offered plenty of aid, which they have repeatedly refused. Additionally, the lack of reporting health and nutrition statistics is concerning for many reasons. First, this most likely means that no one, including the Venezuelan government, knows the extent to which the Venezuelan citizens are suffering. Second, it shows that the Venezuelan government is willing to conceal the level of suffering experienced by its citizens in order to protect their image, instead of asking for assistance; it sends a message that they do not care about the wellbeing of the citizens they are supposed to serve and protect. The UN continues to urge the Venezuelan government to let them send assistance, warning that their situation can become much worse than it already is, but they continue to refuse and push back on any assistance offered and put the lives of their citizens on the line.
Pop Art Explanation Explain by JanBaby, Creative Commons
Introduction
The field of medical anthropology is charged with exploring how cultures determine health outcomes and how health determines culture within a given population. Culture is here defined here as the continuous process by which humans create and communicate shared values, customs, and knowledge within a society; health is here defined as the state and process by which an individual promotes well-being and quality of life. Medical anthropology is especially interested in marginalized populations, exploring how these groups both suffer from health disparities and overcome these disparities through culturally-particular sources of resilience and strength. At the core of medical anthropology’s exploration is the concept of our three ‘bodies’: (1) our physical body, i.e. the body of lived experiences; (2) our social body, i.e. how culture symbolizes and represents our personhood; and finally (3) our body politic, i.e. how our bodies are regulated, surveilled, and controlled over our lifetime (Scheper-Hughes & Lock, 1987). Individuals suffering from any form of violence (direct, indirect, and / or structural) typically suffer worse health outcomes, unless other protective factors (e.g. resilience, medical intervention) can transform this violence.
Of particular importance within the American ‘health culture’ is that of black bodies – how Americans of African descent suffer from higher rates of diseases, illnesses, and sicknesses than their counterparts from European descent. This health-based intersection of nationality, ethnicity, and violence is not only a concern of medical anthropologists – many other academic disciplines are working hard to predict, control, and prevent health disparities within Americans of African descent. For example, I currently manage a health and clinical psychology laboratory at UAB under the direction of UAB Psychology professor Dr. Bulent Turan. Our lab explores the biopsychosocial burden of stigma on health outcomes in African American populations. The question of how culture enacts stress, trauma, and negative health outcomes in minority populations, and how to prevent this from happening in the future, is a huge task – first undertaken by medical anthropology, now including diverse fields such as health psychology, public health, neuroscience, peace and conflict studies, and medical sociology. In honor of Black History Month, this blog post explores how cultural prejudice and hate quietly kills Americans of African descent.
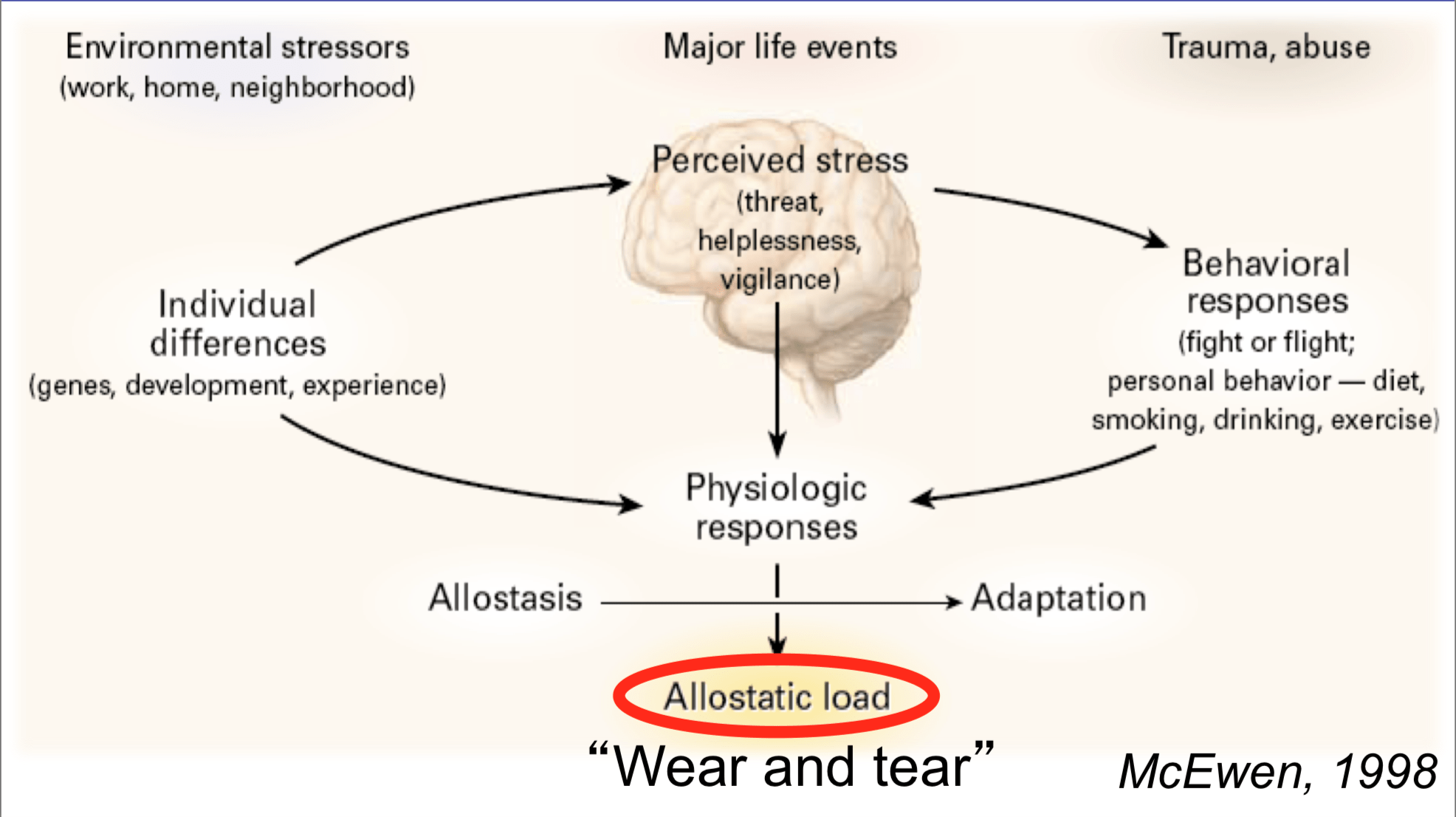
The Allostatic Model of Stress, Author’s Collection
Allostasis and Structural Violence
One of the most prominent and empirically-validated theories to explore the relation between culture and health is that of allostasis, first proposed by Drs. Peter Sterling (a neuro-biologist) and Joseph Eyer (an epidemiologist) in 1988. These scientists and their research team sought to explain how stressful life events impact an individual’s health, first drawing on Walter B. Cannon’s famous dictum of homeostasis– the idea that our bodies attempt to ‘correct’ itself in response a changing environment. Homeostasis explains why, when you step outside on a cold day, that your body begins to sweat to cool you down. However, Sterling and Eyer ran into an obstacle with homeostasis. Individuals react widely differently to physiological stress, and Cannon was unable to explain why this might be the case. Sterling and Eyer proposed that stress over the lifetime creates ‘wear and tear’ within our bodies – higher amounts of stress (for example, chronic stress resulting from racial discrimination) create a higher allostatic load(AL). High allostatic load, according to Sterling and Eyer’s research, results in symptoms including:
High blood pressure / hypertension
High levels of fatty deposits in our blood stream
Blood clotting
Atherosclerosis (hardening and narrowing of arteries)
Suppression of our immune response system
High demands of oxygen by our heart
Having a stroke
Congestive heart failure / heart attack
Allostatic theory (and subsequent empirical support) is quick to add that not all stress is damaging to an individual – eustressoccurs when challenging life events actually make us stronger (for example, the stress your body endures during a challenging workout at the gym). However, chronic and unpredictable stressors are embodied and produce the aforementioned health concerns (this kind of stress is called distress). Therefore, it may be assumed that individuals at a high risk of distress over the lifetime are placed at high risk for negative health outcomes, ranging from momentary physiological arousal to premature death.
A primary driver of chronic, unpredictable distress is structural violence, defined by Galtung (1969) as cultural inequalities (especially lack of access to power) preventing individuals from reaching their full potential. Structural violence is often difficult to pinpoint because there is no one culprit – no one person is responsible for unequal access to healthcare for Americans of African descent; our social system itself is configured to place minorities at a greater risk for distress and lower health outcomes. Farmer (2004) correctly locates several insidious causes for structural violence across cultures, citing historical factors, political forces, latent racism and other forms of unconscious bias, and economic orders as a few examples.
To summarize, here are the takeaways of the complex relation between allostatic theory and structural violence:
Vulnerable populations have unequal access to power within a society.
These populations experience distress due to this unequal access.
Chronic distress manifests in the physical bodies of these populations, leading to high allostatic load.
High allostatic load results in health disparities.
These health disparities go unaddressed due to unequal access.
While indeed tautological, this feedback loop illuminates the vicious cycle many Americans of African descent embody – bodies unjustly assailed and structures unfairly positioned.
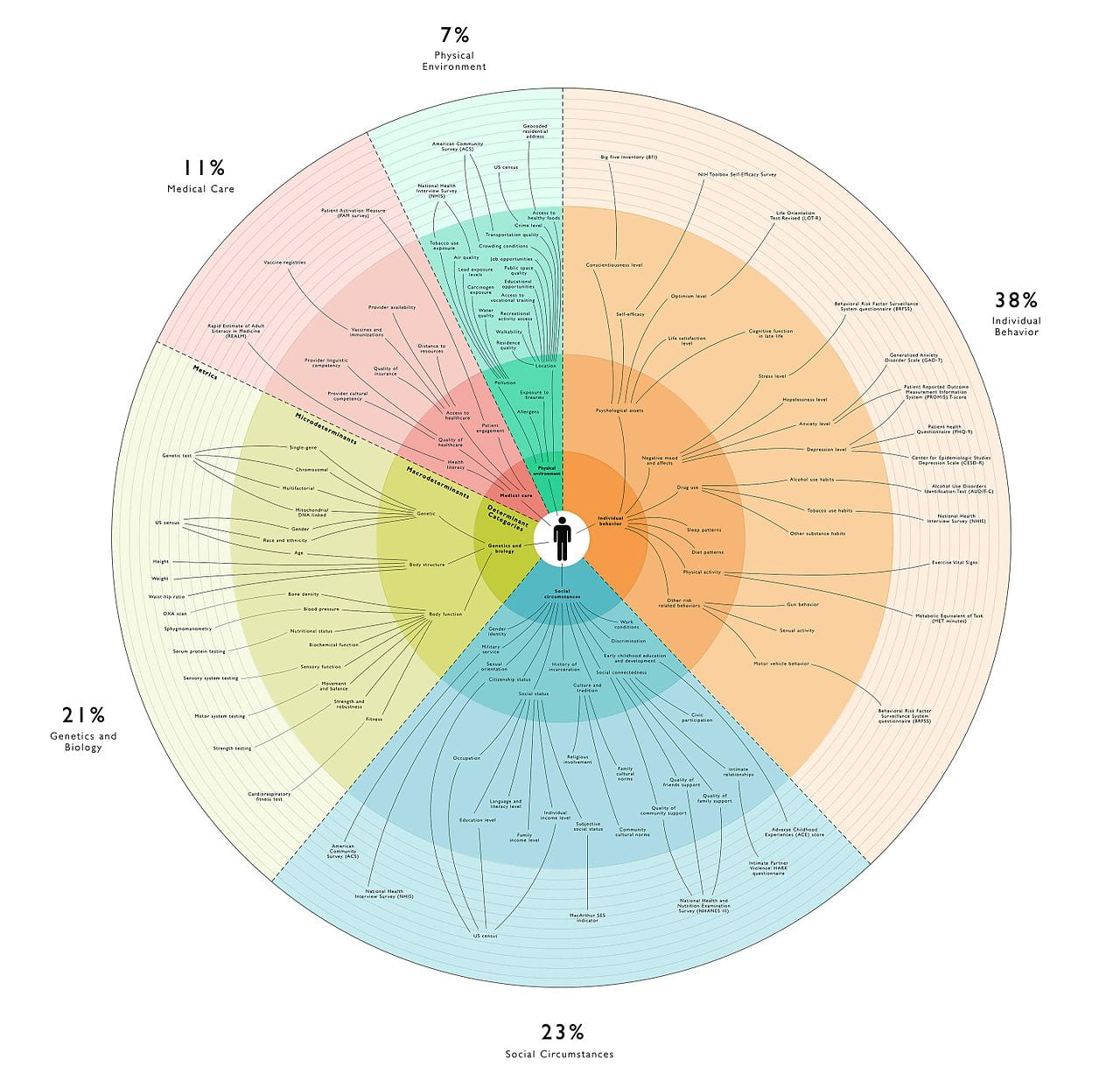
Social Determinants of Health Map by Jsonin, Creative Commons
Black Bodies & Intervention
As previously mentioned, many medical anthropologists conceive of three ‘bodies’ of health: physical, social, and political. The relative health of these bodies acts on one another; it is therefore paramount to address health promotion in a holistic fashion – not only ‘curing the disease’ but also disarming cultural forces that predisposed disease in the first place. Below, I organize threats to and interventions for health in Americans of African descent, according to their physical, social, and political bodies.
Physical
Physical bodies are the stuff of muscles, of skin, of blood. For Americans of African descent, population-level physical health and wellbeing is simply incomparable to Americans of European descent in major ways, including: higher rates of diabetes; of hypertension; of coronary heart disease; of cardiovascular disease; of prostate, lung, and breast cancer; and of asthma-related death. Furthermore, American adolescents of African descent suffer disproportionally from sexually transmitted infections. The infant mortality rate of these Americans is approximately three times higher than infants born to American mothers of European descent. Geronimus, Hicken, Keene, and Bound (2006) demonstrated Americans of African descent experience higher allostatic load than other Americans, controlling for demographic variables, such as education and poverty levels.
According to a systematic review by Crook et al. (2009), there are a few promising avenues for intervention to address physical health in Americans of African descent. These include placing health centers within communities of marginalized populations, using trained volunteer community health workers, and hiring nurses from within the communities of these populations. Additionally, ‘traditional’ healthcare settings (i.e. hospitals) are not necessary to delivery physical health interventions; these interventions can be administered in community centers. Of critical importance here is self-representation – members of marginalized communities empathize with and deliver quality care to members of other marginalized communities.
Social
Our social bodies are reflective of cultural norms, symbols, and values. This body may be conceived of as psychosocial experiences. Our social body is maintained by the attitudes other people have about us. In the case of Americans from African descent, bias, prejudice, and discrimination oftentimes characterize their social body. Clinical-community psychologist Dr. Lyubansky of the University of Illinois at Urbana-Champaign, is quick to assert that this phenomena looks like “racism not always by racists”. In line with allostatic theory, chronic and unpredictable experiences with bias and discrimination induces stress; which, again, causes stress and disease.
Dr. Janice Gassam, applied organizational psychologist, draws on scientific and popular literature relating to social stigma and discrimination and recently published a short guide to disarming unconscious bias. First, we must be aware of our biases; one way to do this is by taking Harvard’s Implicit Association Test. Next, members of majority or privileged populations must make a long-term commitment to reducing bias; this phenomenon will not happen overnight. Next, specific behaviors related to bias must be neutralized; this includes unfair hiring practices and medical maltreatment. Finally, Dr. Gassam asserts that teamwork with members of minority populations can fundamentally disarm cultural bias – evidenced by Edward B. Tichener’s and others’ research on the Mere Exposure Effect.
Political
Finally, the body politic refers to the relation of an individual and her or his political milieu, specifically how the human body is a political tool. The relation is bidirectional as it relates to health and medicine: bodies are both governed by political decisions while also exerting power over the political process. Some bodies (and their corresponding health or otherwise) are prioritized within a political system; other bodies are ignored or violated. A striking example of the violation of political bodies in American culture is voter suppression; we may look to the recent Georgia gubernatorial election and the myriad audacious tactics to keep Americans of African descent out of the voting booth. If individuals cannot vote for policies that may benefit their physical and social health, these individuals do not have political health.
Within the context of the United States of America, voting behavior is the primary way disenfranchised individuals exert political control; it is therefore paramount to empower minority voters so these individuals may elect leaders dedicated to championing causes related to health promotion within marginalized communities. The think-tank Center for American Progress offers five ways to protect the votes of Americans of African descent: (1) eliminate strict voter ID laws; (2) prevent unnecessary poll closures; (3) prohibit harmful voter purges; (4) prioritize African American voters in political outreach; and especially (5) recruit African American candidates for political office. Marginalized Americans must be able to vote for policies and representatives that can break the health disparity cycle.
Conclusion
Observing, predicting, preventing, and controlling health disparities within marginalized populations is an immensely complex issue. As stated in the beginning of this post, medical anthropologists take a cultural standpoint to examine these issues; one prominent theory in this discipline is the systematic examination of ‘bodies’ – how these bodies are affected by health and disease alike. Other fields, such as health psychology, take a more empirical approach – locating specific points of intervention within an individual’s biopsychosocial health processes. This post combines these approaches, explaining how health deficits arise within the communities of Americans of African descent, utilizing allostatic theory and structural violence. To reduce these health disparities, chronic stressors and structural barriers plaguing these communities must be transformed. This transformation begins by accepting a simple fact about black health: the stress from hate can kill you.
References
Crook, E. D., Bryan, N. B., Hanks, R., Slagle, M. L., Morris, C. G., Ross, M. C., Torres, H. M., Williams, R. C., Voelkel, C., Walker, S. & Arrieta, M. I. (2009). A review of interventions to reduce disparities in cardiovascular disease in African Americans. Ethnicity & Disease, 19(2), 204-208.
Farmer, P. (2004). An anthropology of structural violence. Current Anthropology, 45(3), 305-325.
Galtung, H. (1969). Violence, peace, and peace research. Journal of Peace Research, 6(3), 167-191.
Geronimus, A. T., Hicken, M., Keene, D. & Bound, J. (2006). “Weathering” and age patterns of allostatic load scores among black and whites in the United States.American Journal of Public Health, 96(5), 826-833.
Scheper-Hughes, N. & Lock, M. M. (1987). The mindful body: A prolegomenon to future work in medical anthropology. Medical Anthropology Quarterly, 1(1), 6-41.
Sterling, P. & Eyer, J. (1988). “Allostasis: A new paradigm to explain arousal pathology” in S. Fisher and J. Reason (Eds.) Handbook of Life Stress, Cognition and Health. Hoboken, NJ: John Wiley & Sons.
I did something very interesting in my mid-twenties. I asked a few of my family members if they would be willing to be a surrogate if I could not have children. Now, let me preface this by saying I never had any kind of health issues and most women in my family conceived with no problem. My OB/GYN never mentioned irregularities, fibroids, or cysts. My graduate school research had nothing to do with women’s health so I was not inundated with facts and figures. Yet, here I was already concerned and worried (with no discussion of even a long-term future with my partner at the time might I add). My wonderful family, including my mother, tentatively agreed but I am sure were thinking “she has to be joking”. I had never been more serious; I wanted to have options. I did not know what would happen when my womanhood was called out on stage. As women, that is how so many of us define ourselves, right? This is what famed Developmental Psychologist Erik Erikson called generativity: deciding how we will contribute to future generations. In his theory, however, he felt that people usually did not start worrying about this legacy until middle age (or at the very least until a partner was on board), but here I was already thinking about my grandchildren.
About 5 years later, while I was teaching Public Health and Medical Issues in African American Communities, I discovered the documentary series, “Unnatural Causes.” Unnatural Causes delves into the relationship between social conditions and population health. When it came time to discuss health disparities as related to women’s issues, the episode “When the Bough Breaks” was perfect. One statement in the video astounded me: Black women with advanced degrees have worse birth outcomes than White women without a high school diploma. I nearly cried in front of my class. It not only took me back to my concerns in my 20s, but I had just found out I was pregnant with my first child. Would I, a Black woman with a PhD in her early 30s, not be able to carry full-term? Infertility issues, low birthweight babies, and high-risk pregnancies can absolutely influence any woman and family. However, research has uncovered unique circumstances that impact the maternal health of Black women.
Physical Factors
The 2006-2010 National Survey on Family Growth interviewed over 20,000 men and women about family life, pregnancy, infertility, general health, and reproductive health. Chandra and colleagues found non-Hispanic Black women were 1.8 times more likely to report fertility issues compared to non-Hispanic White women. This finding was true among married women as well. It is possible that uterine fibroids, benign tumors in the uterus, affect fertility. Reproductive Science is a relatively young field (compared to Obstetrics and Gynecology which date back to the 19th century), therefore the relationship between uterine fibroids and infertility is far from definitive. However, race/ethnicity is a well-established risk factor for uterine fibroids with Black women developing uterine fibroids at an earlier age than White women. A recent analysis of couples in a reproductive medicine clinical trial found that Black women with uterine fibroids were more likely to miscarry before 12 weeks compared to White women with uterine fibroids. Researchers are trying to identify genetic causes but that will not help the thousands of Black women trying to conceive now.
Psycho-social Factors
Were you ever told babies do not grow in a hostile womb? I heard that at some point in life. During my first trimester, I learned this new information about health disparities in pregnancy outcomes and I was going through a career transition. I was stressed out. Stressors cause the body to release cortisol, which is a necessary hormone when you need to react during intense situations. However, long term exposure to cortisol weakens your immune system and puts you at risk for disease. There is a significant amount of data to support that high levels of cortisol (from continual exposure to stressors) throughout pregnancy can impact the development of your baby. At the same time stress, as a psychological and emotional reaction, is at the center of two of the most common psychological disorders: anxiety and mood.
Anxiety disorders often include fear, tension, nervousness, and dizziness whereas mood disorders often include a sense of hopelessness, fatigue, depression, and an inability to concentrate. Although pregnancy does not increase the likelihood that you will develop either disorder, whether stressed or not, undiagnosed psychological disorders prior to pregnancy can advance further because the symptoms go undetected due to similarities with the normal experience of pregnancy. Dealing with the stigma of mental health issues in the Black community will have to be for another time, different blog! What should a Black woman dealing with certain psychological and emotional symptoms, particularly as stressors, do? Best solutions to deal with stress: walk, yoga, cut out unnecessary activities, watch TV, journal, eat well, and countless other suggestions from books and websites about de-stressing your life. I will admit that I failed miserably in completely de-stressing but I did manage to incorporate a few suggestions over my pregnancy.
How can Black women deal with cultural, historical, and intergenerational stress…the kind of cumulative stress that comes from 400 years of slavery, racism, and discrimination? The pervasive stress that has entrenched itself in the Black psyche? Yes, it is absolutely in there, but it has not just remained in our minds as simple negative thoughts. If that were the case, we could have some sessions of cognitive therapy, learn to counteract those aversive thoughts, and stop perceiving the world as a threat. When one examines racial differences in health outcomes with all things being equal across the racial groups, for example money, education, health care access, and family life, health disparities are still present. Scholars have offered the historical trauma of Blacks throughout the course of US history as an explanation. Could racism not be another explanation for infertility? According to Prather and colleagues, it is the perfect explanation for the social conditions endured by Black women that ultimately influence sexual and reproductive health outcomes.
This is just the tip of the iceberg. There is additional research on the impact of lack of quality healthcare for Black women experiencing fertility issues. Differences in healthcare options affect the recommended treatment and patient understanding of alternatives. There are also observed racial differences in In Vitro Fertilization usage, with money most often the biggest deterrent. Low-income families are very likely unaware that there are grants available to assist with infertility treatment. These are macro-level factors that require changes in resource distribution, medical training, and public policy. And I ask again, how does it help the Black woman trying to conceive now?
As it turns out, I worried for no reason as I thankfully have two healthy and beautiful little girls. I want to ensure that my outcome continues to be the norm rather than the exception going forward. In my opinion, increased awareness of this problem in the Black community will cause a push for more research on racial disparities in fertility issues. Only then will we begin to see changes that will eventually trickle down to support for another young girl in her 20s wondering “can I conceive?”
Dr. Martinique Perkins Waters is an Assistant Professor in the Department of Behavior Sciences at the University of West Alabama. She obtained a PhD in Lifespan Developmental Psychology from UAB in 2010 and since then has taught a variety of courses for Psychology, African American Studies, and Public Health. For over 10 years, Dr. Waters’ research has broadly related to gerontology with specific interest in the social role of caregiving and how that impacts physical, mental, and emotional health.
UAB is an Equal Employment/Equal Educational Opportunity Institution dedicated to providing equal opportunities and equal access to all individuals regardless of race, color, religion, ethnic or national origin, sex (including pregnancy), genetic information, age, disability, religion, sexual orientation, gender identity, gender expression, and veteran’s status. As required by Title IX, UAB prohibits sex discrimination in any education program or activity that it operates. Individuals may report concerns or questions to UAB’s Assistant Vice President and Senior Title IX Coordinator. The Title IX notice of nondiscrimination is located at uab.edu/titleix.