By Grade Ndanu

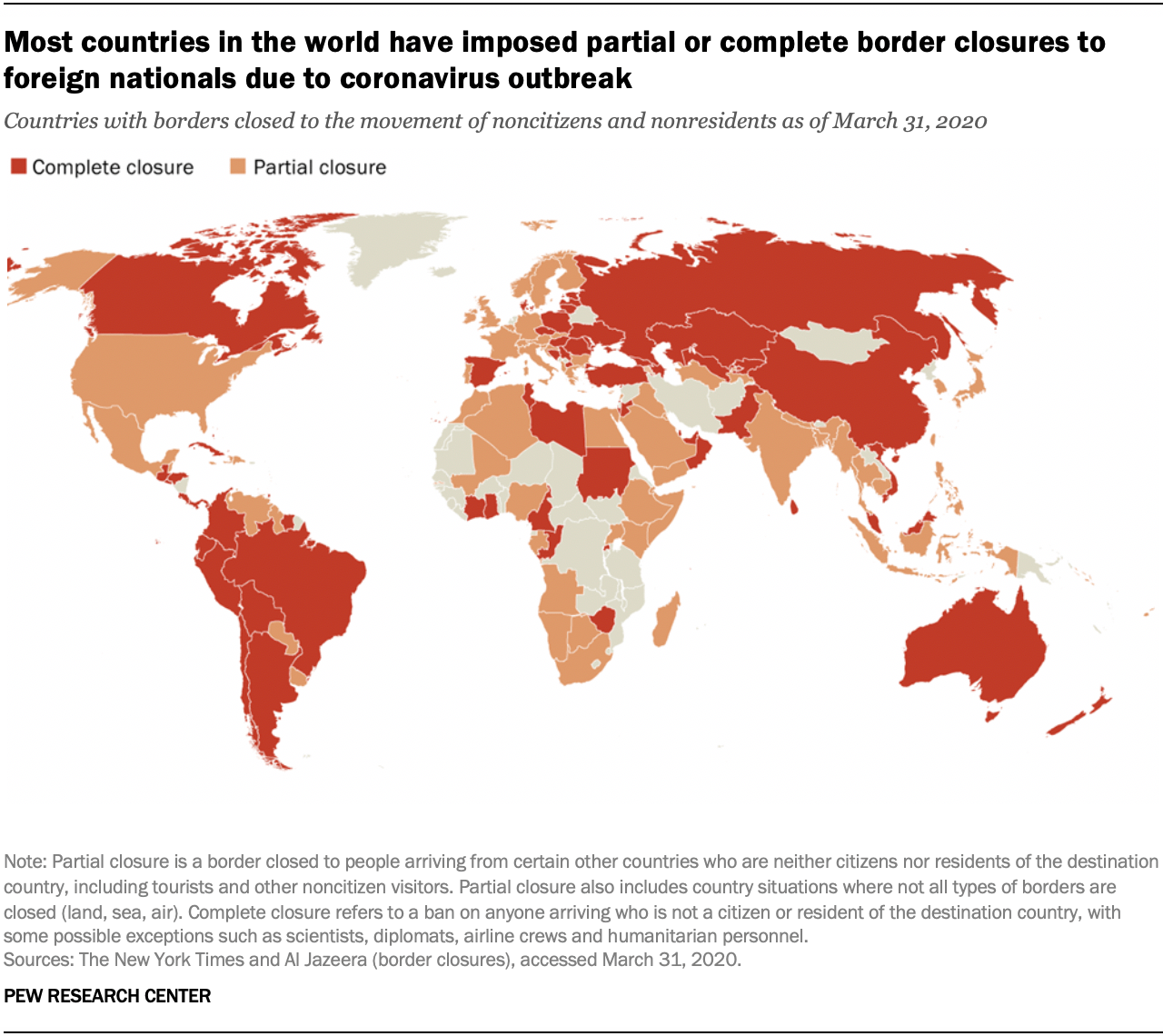
As we watch the news and as I write these lines, the novel corona virus epidemic that started in China, has affected more people than the severe Acute Respiratory Syndrome. Globally on the 30th January 2020 the World Health Organization of the United Nations declared the epidemic a public health emergency of international concern. This defines the outbreak as an extraordinary event which is determined to constitute a public health risk to other states through the international spread of disease and to potentially require a coordinated international response. Countries and airlines suspended travel from affected areas, which is all the countries to be specific and initiated a comprehensive screening at airports.
Wherever we are in the world, we are all living the COVID-19 pandemic. The virus is a public health challenge for the entire global population. Many countries shut down to prevent the spread of the virus. And it came to that day that students never returned to class, employees are working remotely if they can, cinemas are shut, and shops are closed. Basically everything stopped, maybe it’s because the world may have been caught off guard by the size and ramifications of the COVID-19 crisis.
Me being in a unique family, I will share what we are doing to keep safe from the virus and at the same time busy. First we take all the precautions that we are supposed to. We regularly and thoroughly clean our hands with an alcohol based hand sanitizer or just wash them with clean water and soap. All the surfaces including the floor we clean using soap and jick to kill the germs and any bacteria that may be there. We also try our best to practice respiratory hygiene where we cover our mouth and nose when we cough or sneeze. Us being divided in groups that we call families, we tend to help and guide the young ones.
In the centre we are girls of different ages which makes three different groups. The least ages is ten and below. They do coloring and drawing almost daily, and my opinion is, they enjoy which makes them happy. The middle group of ages eleven to fourteen. They usually have their sessions on Thursdays where they are taught about different things for example, last Thursday they were taught about being in a good company, how to stay out of bad company, and how to be a good example. The other group is of ages fifteen and above, and am in that group. We usually have our meetings every Saturday. In this group we are not taught we learn from each other. We are still young to learn about marriage, but yes that was our last topic. Thanks to our mom who acts as our facilitator who we ask very may questions and on top of she teaches us how to bake every Saturday.
Due to the deadly virus, all countries are under lock-down meaning we are all stuck in quarantine. Home is where everyone should feel safe. Being at home means, above all else, being in a place that is dear to you. It should mean protection. But for many children, adolescents, and women, home is a place of violence and abuse. Girls and young women kept at home are safer from the disease but face increased inter-family tensions and an overload of domestic work. Girls, especially those from marginalized communities and disabilities, may be particularly affected and also cutting them off from essential protection services and social networks.
Economic stress on families due to the outbreak can put children, and in particular girls, at greater risk. Girls who are often considered to be adults in the society, experience from very early age the negative social norms that demand they do what women do when they are considered matured for example, cleaning, cooking and child care. Apart from child labor, there is also sexual abuse that is going on. A lot of rape cases before this pandemic the victims were raped by people who they know and also people who are very close to them. Now, we are all stuck with our families whether good or abusive ones. I am really worried of the girls, boys and women who are stuck with their abusive relatives. Even if there are helplines one can’t ask for help because the abuser may overhear the conversation and he may decide to do worse so that the victim may never open up.
Talking of girls, there are girls who are at a greatly exposed to the societal cultural beliefs and practices. In the urban areas, everything seems to have stopped or controlled right now but in the rural areas everything is normal. No lock-downs or restrictions and even no curfews. Meaning that there are so many girls who are undergoing Female Genital Cut, who are helplessly waiting to undergo the cut. Some parents are giving out their daughters hands for marriage. The parents feel that they are free to do anything with their daughters. When schools were on the girls told the teachers what was going on and that prevented many cases of retrogressive cultural practices. Now there is no school where girls would go to their rescue. Am certain these girls feel abandoned.
Activists, social workers, and with the government should be concerned at the potential rise on domestic and cultural violence during this epidemic. While quarantine measures are necessary to reduce the spread of the virus, they should be implemented in a way that guarantees protection for children and women. Measures should be in place so teachers can stay in contact with their pupils. Risk factors should be identified and taken care off. should be visits to the communities, homes, and houses particularly where it is suspected that there might be a girl, child, or a woman in danger.
Let us not just worry about our families and friends. Let us also think of those other people that we don’t know who are vulnerable not only to violence and retrogressive cultural practices but also those who sleep hungry because they luck something to eat. As we remember them in our daily prayers lets wash our hands and take all the precautions that we need to be safe.