Syria and Turkey have been impacted by one of the deadliest earthquakes that have been seen in the Middle East-North Africa (MENA) region. The death toll has surpassed 20,000 and continues to rise considerably, not accounting for the thousands injured. Some of the areas this earthquake has hit are some of the most vulnerable areas in the world. The conditions in both countries are indescribable; with homes destroyed, hospitals at capacity, and limited supplies, the need for help has become critical. It was noted that due to the destruction of the hospitals, and the lack of staff and supplies, patients have had to receive medical attention on the hospital floors. At this point, any type of aid is scarce in both countries. It is vital that everyone supports in any possible way. At the end of this post, you will find numerous links on how to help, whether through donation, reading, reposting, etc. Anything you can do to help is urged. Pass these resources along to your friends, family, colleagues, etc. The most minor contribution makes the most significant difference.
Source: Yahoo Images
What is Happening?
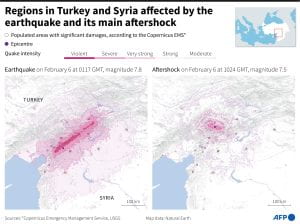
An earthquake with a magnitude of 7.8 struck early Monday morning at 4:17 AM in the Turkish city of Gaziantep, 150 miles away from the Syrian border. This earthquake led to more than 300 aftershocks that rumbled, with one following the initial earthquake just 9 hours later at 1:25 PM and carrying a magnitude of 7.5. Earthquakes are measured using a magnitude scale ranging from 2.5 or less to 8.0 or greater. The Turkey-Syria earthquake reached a magnitude of 7.8 following a shock of 7.5. Meaning this was a significant earthquake that yields severe and destructive damage. This has been one of the worst earthquakes to hit the region since the early 1900s. Along with the destruction of this horrific disaster, the regions are currently facing a winter storm. The temperatures in both Turkey and Syria have dropped tremendously to below 21 degrees Fahrenheit. Rescuers have noted that the weather conditions are so bad that those trapped under the rubble have been found frozen to death.
Source: Yahoo Images
Who is Sending Aid?
Two days have passed since the initial disaster, and the death toll continues to rise. Turkey currently has tens of thousands of rescue teams and aid personnel helping to search for survivors. More than 24 countries have sent aid, help, or rescue teams to Turkey to rescue as many people as possible. With the window closing for the survival of the many lives still stuck under the rubble, the rescue teams are still not losing hope and asking for aid and help. With all the help being given to Turkey, there is an absence found in Syria. Many political and logistical issues hinder aid from being given to Syrians. Since the Syrian Civil War, many countries, such as the EU and USA, have posed sanctions on Syria, and many border points are blocked. At this time, many are urging the sanctions to be removed as it hinders aid to Syria. In times of crisis, we can look to our governments for help, but that is not the case for the Syrian people, which is why it is so critical and necessary to support any in any way you can. Syria is still undergoing and recovering from a Civil War that has been happening for the last 10 years. Many Syrians have been displaced and have become refugees, most residing in Turkey, making the country the world’s biggest refugee host country, with over 3 million Syrian refugees living there. El-Mostafa Benlamlih, UN Resident and Humanitarian coordination for Syria stated: “Sadly, needs are rising rapidly in Syria, and not everyone who requires assistance is visible. Over 75% of all sub-districts in the country are classified as being under severe, extreme, or catastrophic conditions…We must act quickly to ensure more communities do not slide into an inescapable loop of deprivation and negative coping mechanisms.” The areas of Syria affected are some of the worst. Millions of individuals were already displaced in the northwest portion of the country house. With aid in Syria already being scarce, there are many worries and urgencies surrounding the need for humanitarian care.
Source: Yahoo Images
Recommendations:
It is urgent that you can do anything you can to help. Whether that is donating $1, reposting a donation link, or just speaking about it. The current condition these people are living in is unimaginable, so it is vital to help in any possible way. A Syrian journalist has spoken about his experience and current grief. Mohammad Haj Bakri lost multiple family members due to this national disaster. His brother and his three children, his sister and her son, all died under the rubble of collapsed buildings. Although there is international support and awareness for those affected by the earthquakes, I urge you to support them still as much as possible. The aid given to these survivors will be for the current time and post-quake. Below are links to donation sites, articles on how to help, and additional links with information on the conditions.
This article showcases which donation links to use; check out Charity Navigator and GuideStar to ensure that the non-profits you donate to are reliable.
This article exemplifies the urgency of supporting the people of this horrific disaster. This piece explains the stories of those who went through the earthquake, had family members present or had their loved ones die.
A humanitarian aid organization that operates in the rebel-controlled areas of Syria, also known as Syria’s Civil Defense. They are the leading group for helping victims and displaced persons throughout the Syrian Civil war. You can find the link to donate here.
There are countless humanitarian groups accepting donations for those affected by the earthquake. For more resources, check out the links below:
“An individual has not started living until he can rise above the narrow confines of his individualistic concerns to the broader concerns of all humanity.” Dr. Martin Luther King, Jr
Source: Yahoo Images
On this day, January 16, 2023, we remember a man known as the champion of human rights, Civil Rights Leader, Dr. Martin Luther King, Jr., who would have been 94 years old had he lived. As the leader of the Civil Rights Movement, Dr. King dedicated his life to advocating against racial discrimination and injustice. Through multiple death threats, the bombings of his family home, enduring physical attacks and being stabbed, until his assassination on April 4, 1968; Dr. King remained committed to the principle of non-violence. He was only 39 years old when he was killed.
Dr. King believed in the universality of human rights for all and acknowledged that, “Injustice anywhere is a threat to justice everywhere.” What better way to begin a blog about “Human Rights Day” and the “Universal Declaration of Human Rights”, than on the day we commemorate the birth of a man who used his voice, and ultimately risked his life in pursuit of equal rights for all of humanity,
Source: United Nations
Seventy-five years ago, the United Nations adopted the Universal Declaration of Human Rights on December 10, 1948, at a General Assembly meeting in Paris. The UDHR was created to formalize a global standard for human rights across the world. Annually, on December 10th, a day which commemorates the passing of the UDHR, the UN acknowledges this day as Human Rights Day.
What is the Universal Declaration of Human Rights?
In less than half a century, the Universal Declaration of Human Rights (UDHR) has come to be regarded as possibly the single most important document created in the twentieth century and as the accepted world standard for human rights. Referred to as a milestone document in the history of human rights, the UDHR is a collaborative effort of experts from the legal and cultural fields from around the world. The goal was to create a document which rights would be acknowledged globally and would serve as protection for all people living within any nation across the world.
Timeline for the Universal Declaration of Human Rights
On April 25, 1945, on the heels of World War II, representatives from fifty nations met to “organize the United Nations” in San Francisco, California. On June 26, the representatives adopted the United Nations Charter, Article 68. The purpose of this article was for the General Assembly to “set up commissions in economic and social fields and for the promotion of human rights.”
In December 1945, Former First Lady Eleanor Roosevelt was appointed by then President Harry S. Truman to the United States delegation to the United Nations. UN Secretary-General Trygve Lie, appointed Roosevelt to the commission and with the task of creating the formal Human Rights Commission (HRC).
In February 1946, a “nuclear” commission on human rights was created by the United Nations Economic and Social Council (ECOSOC) and its job was to recommend a “structure and mission for the permanent Human Rights Commission (HRC)”.
In April 1946, Roosevelt was nominated to be the chair of the HRC. The ECOSOC gave the HRC three tasks to complete: “a draft International Declaration, a draft covenant, and provisions for the implementation.”
On December 10, 1948, after convening with “representatives with different legal and cultural backgrounds from all regions of the world, the Declaration was proclaimed by the United Nations General Assembly in Paris (General Assembly resolution 217 A).
One might think, we have come far in our efforts to afford equitable attainment of human rights to all people across the world. While we, collectively have made strides, we still have a long way to go to free the world of human rights violations. According to the Institute for Human Rights and Business, listed below are the top 10 human rights issues in 2022.
Redesigning supply chain
Personal Data Tracking & Tracing
Stranded at Sea
Wage Abuse
Office and Work Place
Forced Labor
Climate Change
Racial Matters
Standards Fragmentation
Transition Finance
These issues are reflective of the ongoing and unprecedented impact of COVID-19.
How to Participate in Human Rights Day on December 10th and beyond
Your college experience is full of opportunities to grow and learn, academically, socially and even politically. You will meet people from varying backgrounds and having lived experiences which may be foreign, pun intended, to you. So on Human Rights Day, what can you do to support the initiative? Well, the college interns at the United Nations Association, came up with 10 Ways to support Human Rights Day. Hopefully, you will be inspired to do one.
1. Pass a student government resolution: Work with a member of your student government or student council to pass a resolution in honor of Human Rights Day.
2. Write an op-ed or article in your school’s newspaper: School newspapers can be a great place to talk about the importance of human rights around the world.
3. Stage a public reading: Set up a microphone in your student center or, if the weather’s right, outside and read the Universal Declaration of Human Rights in full.
4. Set up a free expression wall: Set up a blank wall or giant piece of paper and encourage your friends to write about what human rights mean to them.
5. Make a viral video about human rights day: Film your UNA chapter kicking it Gangnam style to celebrate human rights and put the video online: it’ll go viral in a matter of minutes.
6. Start a Facebook campaign: Encourage your friends to change their profile pictures to an individualized Human Rights Day banner.
7. Hand out t-shirts and other gear: If you have the funds, buy t-shirts, sunglasses, or even 90’s-style sweatbands featuring a slogan about human rights to give to your classmates.
8. Coordinate an extra-credit lecture: Work with professors in the history department, the law school, or the international relations program to host a lecture about human rights, and work with other professors in the department to get attendees extra credit—trust us, your friends will thank you.
9. Hold a candlelight vigil or other commemorative event: While it’s important to have fun, human rights are serious business. Consider holding a vigil or other event to commemorate those who have suffered human rights abuses and those whose human rights are still violated.
10. Hold a talent show, dance, or party: Big social events are a great way to bring awareness to an issue, so why not have a human rights-themed party? Free admission if you dress up like Eleanor Roosevelt or Ban Ki-Moon. Also, here are two organizations you can support: Free and Equal and He for She.
Former President of South Africa, Nelson Mandela once said that, “To deny people their human rights is to deny their very humanity.” For the past 75 years, the UDHR has existed to ensure that our human rights are not violated, and if they are that there is accountability on a global stage. We all deserve the right to live freely and uninhibited, the freedom to love who we want and practice the religion of our choice. We must work together as a humanity to ensure that protecting our human rights continues to be a priority.
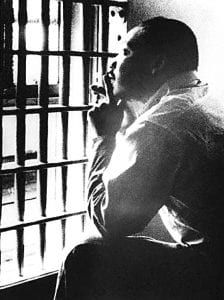
Let us work together to transform his dream into reality. Beyond this nation of the United States, let us work collectively to ensure equal and equitable rights for ALL women, men, and gender nonbinary humans. Protecting human rights was a priority for Dr. King. On November 3, 1967, just a few miles away from this campus of UAB, Dr, King wrote his infamous ‘Letter from a Birmingham Jail” to the Clergymen.
Martin Luther King Jr. in Jefferson County Jail, Birmingham, Alabama, November 3, 1967 Fair use image“While confined here in the Birmingham jail, I came across your recent statement calling my present activities “unwise and untimely… I am in Birmingham because injustice is here… Moreover, I am cognizant of the interrelatedness of all communities and states. I cannot sit idly by in Atlanta and not be concerned about what happens in Birmingham. Injustice anywhere is a threat to justice everywhere. We are caught in an inescapable network of mutuality, tied in a single garment of destiny. Whatever affects one directly, affects all indirectly.”
Dr. King reminds us that “The time is always right to do what is right” and that we as a humanity must ensure that the single garment of destiny is threaded with equal rights for all humans for this is the only true way forward. In the spirit of Dr. King, we must work to ensure that the rights of ALL humans are acknowledged, respected and protected by law, and not just on Human Rights Day, but every day, and everywhere across the globe.
My mother is the youngest of 5 Indian daughters, all of whom are PhDs, professors, researchers, and educators. My grandfather, a lawyer, raised her, and like clockwork, he repeated that knowledge is akin to clay, a necessary foundation for anyone’s house of decisions, thoughts, ideologies, and actions. Because of this, nothing was more important than my education and, later, my brother’s education.
The right to knowledge that my upbringing revolved around is synonymous with the right to choose, the freedom of expression, and the right to read – all rights outlined directly or indirectly in the United States Constitution and subsequent Supreme Court decisions justified by the First Amendment.
Despite the First Amendment’s protection, book bans in schools are threatening this right to knowledge for students. Within the last 2 years, books of all literary and historical acclaim, including modern literature, have been banned at an unprecedented rate in an alarmingly organized manner in public school districts.
When people lose their right to this knowledge and succumb to political pressure, it will be a day in history representing humanity losing its most powerful tool to stand up for justice.
Woman looking through book spines in a bookstore. Source: Unsplash
Like all examples of institutional limitations, the most influential books, which have the potential to cause revolutions, are also the most restricted. Uncle Tom’s Cabin by Harriet Beecher Stowe was banned in the Southern United States in 1852 and is traced back as the first example of a book ban. Stowe, a ferocious abolitionist in the North, wrote this book prior to the Civil War to rally abolitionists and swing individuals against the South’s slavery. Since the Constitution was written, Northerners decried the South’s defense of slavery. Uncle Tom’s Cabin was a powerful tool that amplified the voices of abolitionists across the country; they believed that slavery was a legal injustice in the Constitution that needed to be removed. Plantation owners, however, were able to pull strings and remove the book from circulation in the South, fearing the loss of economic and racial security that slavery gave them.
A hand fisted upward with a rope wrapped around the wrist. This is a symbol of Juneteenth, the national celebration of the emancipation of slavery. Source: Unsplash
One of the first instances of controlling students’ access to books was after the Civil War. The Southern United States restricted access to textbooks that painted the South’s intentions and actions poorly amid the Civil War. An advocacy group in the South referred to as The United Daughters of the Confederacy felt that the control of what information their children were learning during school was beholden to the rights of parents. In 1954, they removed The Rabbits’ Wedding, a novel centered around a black rabbit marrying a white rabbit. They feared it would normalize interracial marriages, a taboo act at the time.
In direct opposition to school censorship, the Supreme Court ruled that school boards “cannot remove books from school libraries just because they dislike the ideas contained in those books” in the landmark 1982 Island Trees Union Free School District v. Pico case. The Island Trees Union Free School district removed titles it deemed “anti-American, anti-Christian, anti-Semitic, and just plain filthy.” In conjunction, the Supreme Court also ruled that students retained their First Amendment rights to the freedom of speech and expression in school in the Tinker v. Des Moines case. If we follow the court, censorship is illegal in the U.S.
Young students listening to a teacher or speaker in their school classroom. Source: Unsplash
Over 1600 books have been banned nationwide. Most of them are fiction and illustrate the lives of the LGBTQ+ community and people of color. In the past, book bans originated from a small scattering of parents making personal requests to remove a few books from circulation or restrict their children from reading them. Today, the opposition is still a minority, but they are organized with structured advocacy groups taking center stage at school board meetings demanding specific books to be removed from circulation. Some of the most banned books, like The Hate U Give by Angie Thomas, is a novel centered around a black teen who witnesses her black friend get shot by a white police officer. Another is The Absolutely True Diary of a Part-Time Indian by Sherman Alexie, which discusses the life of a Native-American teenager aspiring to be a cartoonist in an all-white school. Essentially, the most targeted books discuss life outside the white picket fence of middle-class white suburbia.
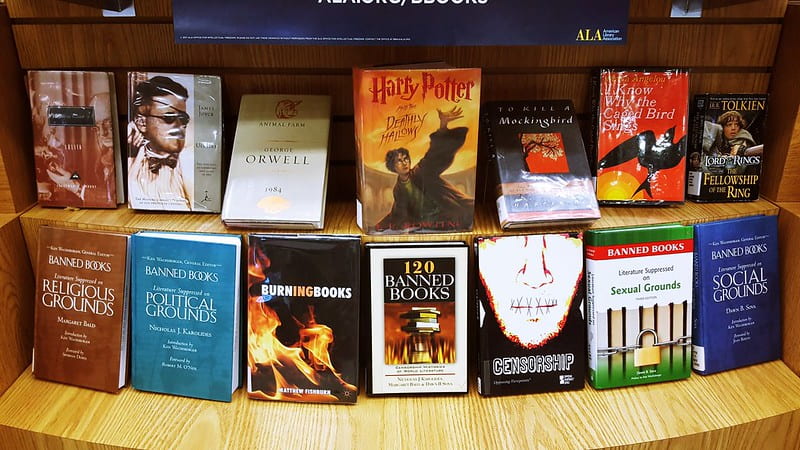
A collection of books that have been banned or proposed to be banned on a wooden shelf. Source: Flickr
What do supporters of book bans hope to achieve?
Ellen Hopkins, the author of the Young Adult poetry verse book Crank, is one of the most banned authors in the United States. She feels that parental rights and concern for children’s safety are a smokescreen behind anti-book advocacy groups’ motivation. Hopkins implores that books provide kids with the opportunity to solace in information about their identity and find consolation that they are not alone. They also prepare children for life in the real world by exposing them to situations they might otherwise encounter. Thus, books are a tool for the development of holistic decision-making skills. Removing these opportunities leaves kids with little chance to make better decisions when confronted with situations they are not familiar with. If the child is BIPOC or queer, removing books that have become championed narratives from the respective community isolates them and invalidates their experiences.
Parents often find these books on lists circulating online and present them to their children’s school districts claiming there is offensive or inappropriate content that compromises their children’s innocence. PEN America has found that parents who appear at the board of education meetings en masse and are armed with arbitrary lists of books have rarely even read the books to understand their significance. Descriptions of “obscenity” are affixed to titles as a fearmongering tactic to cultivate reprobatory characterizations of these books as they quickly make their way through advocacy groups’ websites and Facebook to radicalize those that come in contact with these types of posts. Such inflammatory language, which is not considered legally acceptable, elevates a small minority of individuals into a vocal majority to force school boards to comply.
A group of adults in a meeting with notebooks listening and taking notes on the speaker. Source: Unsplash
Solutions to Book Bans
Banned Books Week stands as a beacon of hope against the dark wave of censorship. This week celebrates suppressed voices in literature and amplifies authors’ messages through community outreach, and fosters national collaborations. However, progress is made in consistent steps, not leaps.
On a smaller scale, there are many tools you can use in your community to combat literary censorship. Community members, feed off each other’s ideologies, and to mellow the extreme views of this vocal minority, the first step is to provide outlets for conversation. The vocal minority advocating for book bans can be confronted and overcome when faced with the majority opposed to them or their thinking. You can make your presence felt at school board meetings. Show up and voice your opinion and advocate for others to do so over social media. Vote for your local boards of education, library boards, and city council elections. If you want to, run for these board positions yourself or directly appeal or lobby your legislative representatives and defend the importance of all content in books. Unite Against Book Bans also provides communities with toolkits that include essential questions and moderate answers that consider the argument of parental rights while protecting the First Amendment.
In all, I am grateful for the circumspection that my mother and my family’s push for education provided me with. Not only hard skills, but also the ability to think for myself, to derive my own opinions, and to be mindful of how I act and react to new information. My freedom to read and speak gave me a powerful voice that must be available and fostered in everyone.
An image of a tightly packed women’s prison. Source: Soumya Misra (Nursing CLIO) via Yahoo Images Public Domain
This is a continuation of the conversation about the Alabama Prison Crisis as exposed by Mary Scott Hodgin in her podcast, “Deliberate Indifference.” If you have not read the previous blog post on this topic, “The Ongoing Alabama Prison Crisis: A History”, it is recommended that you do so. Also, if you would like more information and details regarding this topic, please listen to the podcast, “Deliberate Indifference,” by Mary Scott Hodgin. Now, without further ado, let us jump right in from where we left off.
In the previous blog, we focused on the history of prison systems in America, and particularly, some of the legislations and ideologies that laid out the foundation for the correctional institutions we know today. We explored in detail the convict leasing system that helped rebuild the infrastructure of the Antebellum South following their defeat in the Civil War, and the racialized laws and legislations that disproportionately landed Black and Brown people in prison over their White counterparts. The War on Drugs era followed by the Tough on Crime era landed hundreds of nonviolent offenders in prison, serving longer and harsher sentences and life without parole. While our focus in the last blog was more nationwide, it was necessary context to set the stage to better understand the realities that face the Alabama prison systems focused on in this blog.
The objective now is to look deeper into the conditions of the penal system in Alabama, the lawsuits they faced in 2017, and the most recent one in 2020, how the pandemic exacerbated these conditions, the prison strikes that took place within these prisons, and some ways to move forward to bring about actual change – change in the mindset of our fellow Alabama voters, and a shift in the way the prison population is viewed and treated as a whole. We will look at some groups that are trying to do just that, from organizations like Alabama Appleseed and the Offender Alumni Association to religious groups and other educational groups that sponsor programs within the prison system to provide opportunities for higher education to the imprisoned population.
Prison Conditions
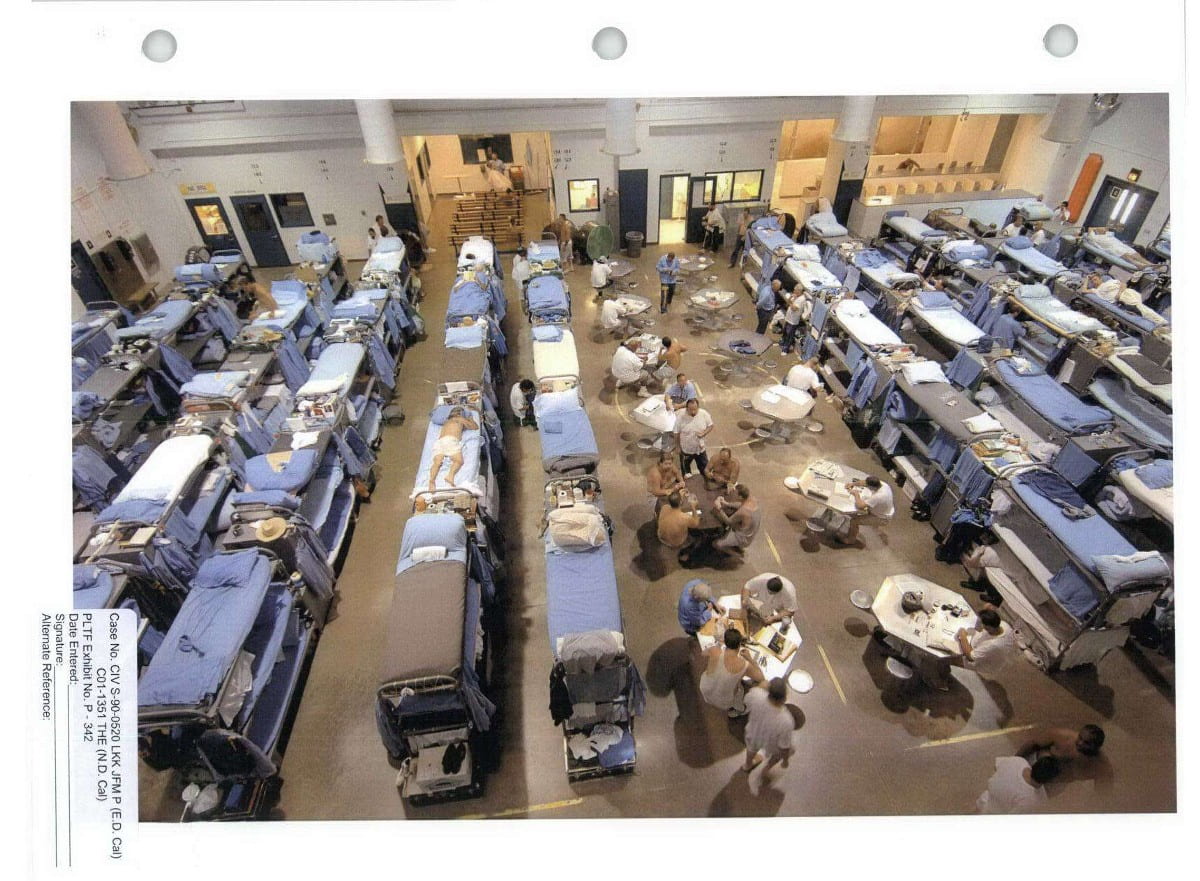
An image depicting a dormitory-style housing unit. Many of Alabama’s prisons are structured this way. Source: Yahoo Images via ACLU
While exploring the most recent reports that resulted from the federal investigations of Alabama’s prisons, there were many similarities in the reports. While the problems of understaffing and overcrowding were expressed in detail, (which will be discussed below), there was also extensive observation of the living conditions inside the prisons. What the investigations revealed was shocking, and despite having been advised to address these issues even in the 1970s investigation of Alabama’s prisons, the conditions had not improved. Rather, it had deteriorated even more due to the consequences of staffing and crowding issues.
Both reports extensively provide detailed examples of violent outbreaks within the prisons, between prisoners, and even at the hands of prison staff targeting the prisoners. Many such incidents go unreported, and others have even ended in the death of the imprisoned person. One of the things that contribute to this violence is the structure of the prison itself. Many of Alabama’s prisons are fashioned in a dormitory-style of housing units instead of the individual cell units depicted in popular culture. These housing units are essentially enormous halls that are secured on the perimeters, with bunk beds piled into the room as close as they can fit. With little to no privacy, and jampacked in tight spaces, people can get easily agitated, and this can lead to violence. Due to the overcrowding issue, many people are even expected to sleep on the floors, which can be unsanitary and uncomfortable. Due to the continuous staffing issues these prisons face, these large units may go unguarded for long periods of time, sometimes even entire shifts.
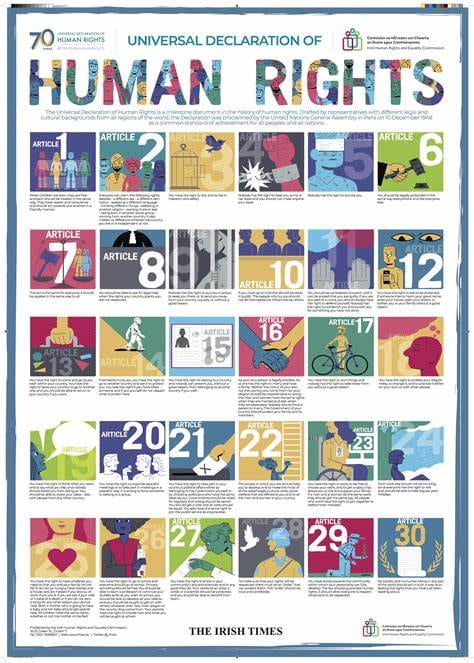
This puts both the inmates within the units at risk for violence, and the prison staff who, to the incarcerated individuals, represent the authority from which these conditions are sanctioned. Even still, many officers, due to the understaffing issue, have overlooked contraband possession (such as drugs or cell phones), deciding to pick and choose their battles in an already tense environment. As a result of all these issues, corruption is rampant within the prison walls, and many prison staff, according to narratives from both reports, take advantage of this tense environment to assert dominance over prisoners with increased brutality. People who are incarcerated are not viewed by society as individuals with their own pasts and presents. They are only viewed as “criminals,” remain invisible to society and are dehumanized. Regardless of the crimes that a person commits, they are at the end of the day, still, people, who deserve dignity and basic human decency. As an institution of the state, prisons are legally responsible for providing a safe and secure environment for people who are incarcerated to serve out their sentences as punishment. The American Constitution does not support “cruel and unusual punishments”, and under the Universal Declaration of Human Rights (UDHR), the rights of imprisoned individuals are fully supported.
An infographic that lists the universal rights protected under the Universal Declaration of Human Rights (UDHR). Source: Irish Times via Yahoo Images Public Domain
2017 Federal Investigation
In the previous blog, we focused on how the prison system of Alabama has been under federal investigation nearly 50 years ago in the 1970s. Unfortunately, the conditions outlined in those reports were never fully addressed, and the issues that were highlighted have only been exacerbated over the years. In September 2017, the Department of Justice from the federal government toured one of Alabama’s prisons, Bibb County Correctional Facility, for their official investigation of prison conditions in the Alabama penal system. What they uncovered was outlined later in a report published in 2019, stating over 50 pages worth of evidence against Alabama, and the minimal expectations the federal government laid out for Alabama to achieve, both short-term and long-term.
The report is prefaced by the fact that these concerns were underlined within a week of their investigation. According to the report from the observations made in 2017, the Alabama correctional facilities faced a myriad of issues, including an overcrowded prison population, with dangerously low staffing, issues of contraband entering the prisons, and a host of observations pertaining to violence within the prisons, including physical, mental, and sexual violence. As discussed in the previous blog, these overcrowding issues come from the various legislations that were passed, increasing the lengths of sentences, criminalizing drug abuse and mental health issues (instead of treating them as medical issues requiring rehabilitation and treatment), and incorporating mandatory sentencing minimums and three-strikes laws. Along with identifying the concerns stated above, the report also deemed the penal system’s inadequate protection of its inmate population from harm, violence, and death, a failure. The report discussed at length how, along with unsanitary living conditions, there are dangerous weapons and drugs that are circulating within the prisons, making them unsafe for both the incarcerated people, as well as the officers who work there. This in turn is both caused by and exacerbated by the issues of overcrowding and understaffing within the prison walls. With fewer officers to supervise the dormitory-style prisons in Alabama, incarcerated people are packed together to fend for themselves.
While not all people locked up in prison are violent offenders, studies have shown that desperation, (which is rampant in these prisons), can lead to violence, distrust, and increased criminal behavior within the population. While the study referenced focused on populations outside of prisons, it is safe to assume that these results are only amplified within the prison system. The people within are both desperate and already undergoing punishment, which means that even the threat of punishment is not a deterrence from committing these violent acts. This also means that with fewer officers to supervise the dorms and halls of the prison, the overall violence within the prisons is increased, making it dangerous for the entire prison population.
As explained in both the report by the federal investigation, as well as the podcast by Mary Scott Hodgin, there were at least 11 men that died in 2019 alone due to the increase in violence within the Alabama prisons. To make matters worse, the federal investigation also found that the Alabama prison system’s record-keeping on these incidents and others was inaccurate, finding that there were many incidents that went unreported, and even many deaths misclassified as due to natural causes or medical reasons rather than due to the violence found within the prisons. If you count the total number of deaths within the inmate population in 2019 classified as natural causes or otherwise, the number is as high as 119 deaths.
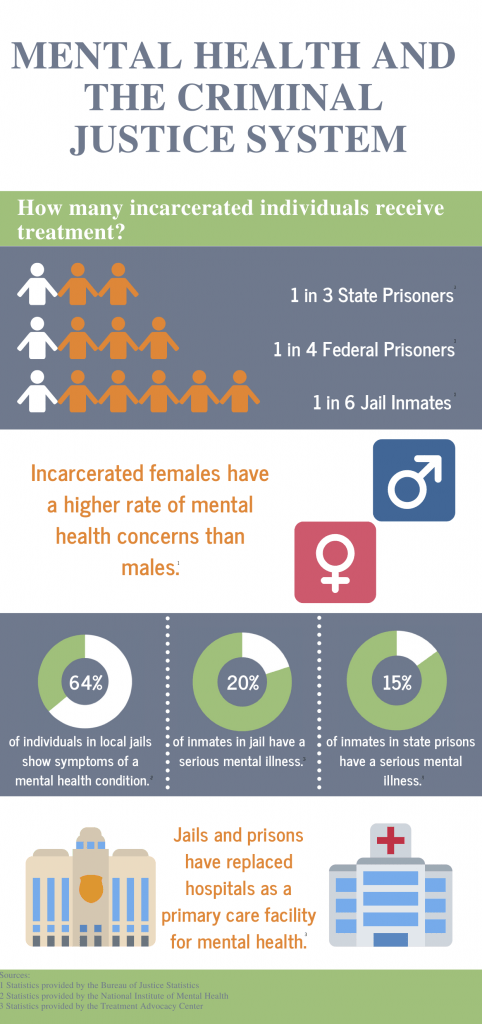
An infographic providing statistics on mental health in the prison system. Source: Cabrini University via Yahoo Images Public Domain
In addition to the misclassifications and incidents not being reported, Hodgin also details in her podcast the inadequate mental health care offered to incarcerated individuals within Alabama’s prisons. This can lead to an escalation of violence, and abuse of drugs, and place incarcerated individuals dealing with mental health issues in dangerous situations. Without the proper medical attention required to treat these individuals with mental health illnesses, prisons can become a charged environment that can exacerbate their conditions, making them more vulnerable to both becoming victims of violence, as well as the perpetrators of the violent acts. Unfortunately, because people with mental health issues are four times more likely to be imprisoned instead of receiving treatment and care, many individuals in prison already enter the system without knowing how to follow social norms. This can put them in danger of being abused by officers and other imprisoned individuals alike, and without proper care, their conditions can become worse, and at times, can end in death, either at their own hands or at the hands of another.
Another major topic of concern addressed in the report is that sexual abuse and sexual violence. Sexual violence is rampant in Alabama’s prisons, and this issue is exacerbated by the understaffing issue present within these facilities. With fewer officers staffed to care for increasing numbers of imprisoned people, there is less monitoring and supervision taking place, creating a breeding ground for violence, both sexual and physical. Much of the sexual abuse either go unnoticed, or unreported by staff members, and while the victims can report these incidents too, many choose not to for fear of retaliation or feelings of shame. Their fear is not unsubstantiated, as many accounts have been provided in which sexual assaults took place in retaliation to the victim’s reporting of a previous sexual assault. In addition to the low staffing numbers, many of the facilities in Alabama are constructed in a dormitory style, meaning that imprisoned individuals are grouped into a big hall rather than individual cells. This can be challenging for clear visibility of each individual inside the prison and their whereabouts. At times, only one or two officers may be in charge of the entire unit, and sometimes, the incarcerated people go unsupervised.
Many incidents of sexual assault occur as a result of “drug debt”, where an incarcerated person owes another incarcerated person money for drugs or other contraband and does not pay. There have even been incidents where family members of people who are incarcerated have been extorted for money, with the threat of sexual violence against their imprisoned family member. Many victims of sexual abuse within the prisons also alleged that these instances occurred after the victims themselves were drugged or held at knifepoint. While much of this goes unnoticed by the prison staff, some reports that do manage to document these incidents have even labeled sexual assault as “homosexual acts” rather than nonconsensual sexual abuse. People who are incarcerated that belong to the LGBTQI+ community are even more vulnerable to sexual violence simply for their identity. Unfortunately, many of the officers in charge of ensuring that the prisons comply with the Prison Rape Elimination Act (PREA), are not even aware of who among their incarcerated population belongs to the LGBTQI+ community. The PREA flags the LGBTQI+ population as being most at risk for sexual crimes, and the PREA managers in the Alabama Department of Corrections are not fully complying with the standards set by the legislation.
After identifying and explaining the various issues the Department of Justice found within Alabama’s prison system, the report argued that these conditions violate the constitutional rights of the incarcerated people, and as such, provided some bare-minimum measures that Alabama should take immediately to avoid a federal takeover of the prisons. These remedies included addressing the issues of overcrowding and understaffing, the rampant violence (both physical and sexual), the access to contraband, and the living conditions within the facilities. In addition to these short-term measures, the report also suggested some long-term measures to implement, including – among a list of other things – better incentives to improve staffing issues, improved systems to track, record, and address issues of violence, and more regulation over prison conditions and treatment of the imprisoned population. Alabama closed down one prison after this report (Draper Correctional Center) and closed a particularly harmful “behavioral modification unit” or “hot bays”, (where incarcerated individuals are held as punishment for violence and drugs within the prison) at Bibb Correctional facility. While these closures were a good place to start, they should be in no way, the only solutions to the long list of problems outlined by the report following the federal investigation. Unfortunately, Alabama, as expressed in the report itself, has been “deliberately indifferent” to these situations, and as a result, experienced yet another investigation in 2020.
2020 Federal Investigation
An image of an overcrowded cell colored in red symbolizes prison violence. Source: ProPublica via Yahoo Images Public Domain
The 2020 report from the Department of Justice’s investigation into Alabama’s prisons found similar problems echoed in the 2017 investigation they conducted. As mentioned in the 2017 report, the 2020 report also addressed issues of overcrowding of prisoners, stating that all of Alabama’s 13 prisons held thousands of people over the capacity they were designed for, making Alabama’s prisons among the most overcrowded prisons in the nation. This report also referred to the dangers of not having adequate staff members to care for and run these overcrowded facilities, this time focusing on how these staffing and overcrowding issues have led to an increase in officers using excessive force against the incarcerated individuals, further aggravating the violence that exists within the prison walls. This issue of excessive force is further examined in the report, claiming it is a violation of the Eighth Amendment to the Constitution of the United States which outlaws cruel and unusual punishments against imprisoned people.
The 2020 report details the many reasons why officers use excessive force against people who are imprisoned. Unfortunately, many officers have been known to use violence and excessive force to “handle” a situation, even in times when there is no physical threat to the officer, and even when the incarcerated people are complying with the given orders. This has the tendency to escalate the situation, placing both the incarcerated individual and the officers in danger’s way. The report provides various examples of such incidents where the imprisoned people are reported to be complacent with the officers’ instructions, even handcuffed without ways to fight back, but have still been beaten, tortured, and abused inhumanely. These officers filed false incident reports claiming that they did not engage in such actions, and even after investigations of the incidents, the officers did not face any legal consequences or disciplinary actions for their behavior.
At times, excessive force is used by officers as a form of punishment or retribution for disrespecting the officers or reporting them. The 2020 report describes multiple incidents where excessive force was used against incarcerated people simply for not following the specific directions laid out by the officers. One incident includes an imprisoned person being physically abused and forced to eat all the leftover chicken for simply wanting some extra food. Other incidents outline the use of chemical sprays to punish incarcerated people or as a form of retribution for not following verbal orders. Chemicals sprays are used even in times when the imprisoned people do not pose any physical threats to the officers. Finally, many officers also use force to simply assert dominance and inflict pain on their charges, something that not only endangers the people involved (both officer and incarcerated individuals) but also causes the incarcerated individuals to distrust the officers in charge, escalating the tensions between the two groups.
All these incidents are violations of the eighth amendment, and while many of the investigations that these incidents resulted in agreed that there was no justification for the use of excessive force in any of these outlined incidents, the officers faced little to no disciplinary actions for their conduct. The Department of Justice also included this issue in their report, arguing that unsurprisingly, officers either fail to report or inaccurately report incidents where excessive force is used. Many times, excessive use of force is investigated internally and recommended for an I & I investigation (Investigations and Intelligence unit of the Alabama Department of Corrections in charge of investigating misconduct by prison staff). Unfortunately, the report declares that of all the incidents recommended to the I&I unit, only 40% of them are actually reviewed. To make matters worse, many of the cases that are investigated by the I&I unit, where excessive force has been confirmed, are seldom referred to be criminally prosecuted. This means that many of the officers abusing their authority and misbehaving with incarcerated individuals go unpunished for their conduct. Many more of the incidents where excessive force is used go unreported, with only the victim’s bruises to bear witness to the incident. For fear of retaliation, many imprisoned persons go without reporting the abuse they face at the hands of officers. If the victim does not cooperate in the investigation, the incident is deemed “unsubstantiated”, and the investigation is closed.
Following their investigation, the federal government proposed a list of measures that Alabama’s Department of Corrections needs to take in order to fully comply with federal regulations for correctional institutions. These immediate measures included the need for more I&I investigators, a better system for victims of abuse from officers using excessive force to report their incidents anonymously and independent of the prison’s authorities, clear procedures for accountability for officers, and better documentation and investigations of incidents where excessive force is used.
COVID-19 and Its Impact on the Prison Population
A cartoon depicting a prisoner digging with a shovel, with a caption underneath reading: “I’m not escaping. I’m just trying to get tested for Covid-19.” While this image was referencing the protocols followed by Mississippi prisons, this was essentially the same in Alabama’s prisons as well. Source: Mississippi Today via Yahoo Images Public Domain
In addition to these inhumane conditions the imprisoned population experience that violate the basic human rights of incarcerated people, the outbreak of Covid-19 greatly amplified this issue, and soon, the prisons became a contagious and deadly environment for both the prison staff and their charges. With little to no access to adequate healthcare and deteriorating mental health caused by the conditions of their environment, people who are incarcerated are especially vulnerable to disease outbreaks. On the national level, according to a study conducted in 2020 by the American Medical Association, people incarcerated were five times more likely than people living outside the prison system to be infected by the virus, and the death rates among prison populations were higher than the national average at the time. Making matters worse, due to conditions of overcrowding inside the prisons, the outbreak was especially dangerous, as incarcerated people were unable to adequately quarantine and unable to maintain safe social distance between each other. There was also the probability of prison staff bringing the virus into the prisons from the outside world, and also recirculating the contagion within the prisons back into the larger society. A UAB publication by the School of Public Health declared the prisons a “petri dish for COVID-19”.
To add to this problem, the prisons were notoriously unsanitary, meaning that preventative measures such as maintaining clean spaces and washing hands with anti-bacterial soaps, were impossible to maintain. Furthermore, understaffing issues complicated this situation, as those who were infected were either neglected until conditions were too bad to ignore, or they were provided with inadequate healthcare measures. In Alabama, a unique situation further complicated the negative consequences of the pandemic. A large portion of Alabama’s prison population belongs to the older age groups due to the strict and long sentencing laws of the state, and the fact that the pandemic was considered to be even more dangerous for elderly people further put people incarcerated within Alabama’s prisons in jeopardy. Access to healthcare within the prison system makes this issue life-threatening, and despite the urgency from the American Medical Association to include the prison population in the vulnerable communities list for vaccinations, the Equal Justice Initiative reported that Alabama’s prisons denied its incarcerated people vaccinations. While some prison staff received vaccines, they were not required by the state to be vaccinated to work in the prisons, continuing to place the lives of incarcerated individuals in peril. As a result of inadequate protective gear (such as masks), and negligent behavior on part of the state and the prison staff, the prisons in Alabama encountered a large number of Covid-19 deaths.
Alabama Prison Strikes
A group of people protesting prison conditions and calling for the protection of the rights of incarcerated people. Source: Occupy Oakland via Yahoo Images Public Domain
After living through the grave conditions of the pandemic, and witnessing the unchanging environment within the prisons, the incarcerated individuals decided it was time to take matters into their own hands. In September of 2022, incarcerated people from all of the 13 prisons in Alabama began striking against the prison conditions they endured. They argued that the prison system was violating their basic human rights, provided inadequate healthcare, and did not in any way prove to be a place of rehabilitation for the imprisoned population. Instead, they initiated a strike, refusing to work their prison jobs (such as in the laundry department and the maintenance department) that they did not receive compensation for, called for improvements in prison conditions, and demanded reforms to the harsh sentencing laws currently in effect in the state of Alabama.
While imprisoned persons are demanding to be treated fairly in prison, the governor of Alabama, Kay Ivey, insisted that the demands of the prison population were “just unreasonable,” maintaining that the new construction of the two mega prisons in Alabama would solve all these issues of understaffing and overcrowding. These mega prisons, built with the use of funds designated to the state for pandemic relief, (causing public debate on this controversial subject), are supposed to provide more space for the overcrowded prisons in Alabama, and reports have surfaced about the possibility of hiring more officers for the newer mega prisons. This project will receive a total of over $1.2 billion in funding, of which $400 million comes from the pandemic relief funds.
What is vital to include here is that while these two new prisons will provide more space to house incarcerated individuals, (up to 4,000 in each), these prisons are replacing existing prisons with newer technologies and facilities. While this may seem like an improvement in some prison conditions, (such as more security and cleaner, sanitary units), it does not solve issues of overcrowding or staffing issues. The massive budget awarded to this project, instead of going toward building two mega prisons, could have been used more wisely to address the core issues of society that increase crime and criminality within its community. In addition, certain legislation and reforms could have been passed to overturn the harsh sentencing laws that exist in Alabama today. This would have solved both the issues of overcrowding and understaffing, as with fewer people being incarcerated and more people qualifying for parole, the total amount of people within the system would decrease, which would also lead to a decrease in the number of incarcerated people the prison staff is responsible for. A decrease in the prison population would also lead to a decrease in violence and more space for each individual within the prison walls.
Existing Resources
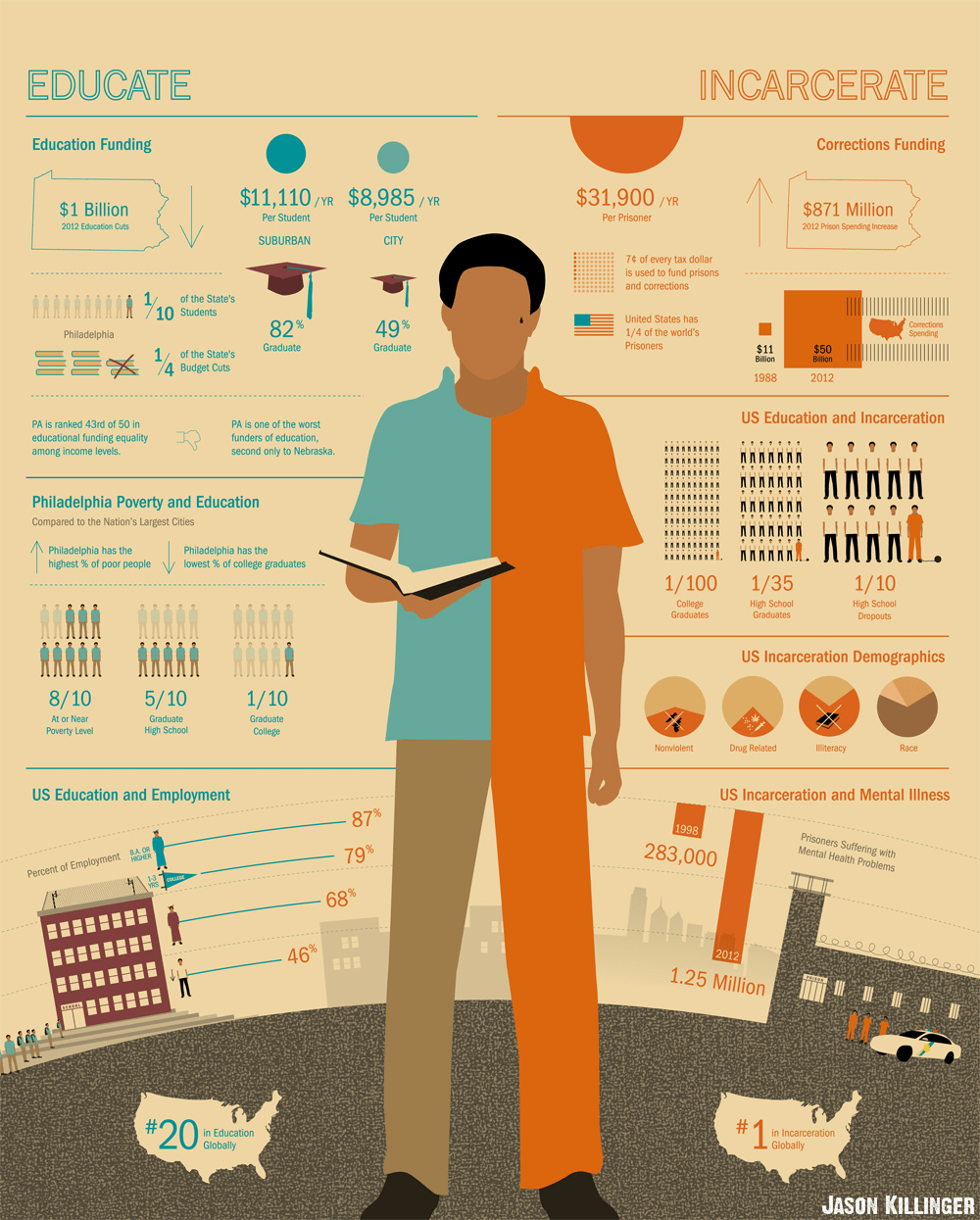
An infographic depicting the difference between education and incarceration. Source: Yahoo Images via QEDfoundation.org
There are many organizations that have attempted to address both the various issues that incarcerated people face within the prison system and those face as they re-enter society after completing their sentences. These organizations include Alabama Appleseed, Offender Alumni Association, Shepherds Fold, One Roof, and Aid to Inmate Mothers. Alabama Appleseed, which belongs to the national Appleseed Network, is a Center for Law and Justice that focuses on equity and justice, and research around prison reforms in Alabama’s penal system. The Offender Alumni Association, recognizing the importance of human connection, focuses on providing support and engagement within the prison walls, and community and stronger familial relationships outside, all while aiming to end the stigma around imprisonment. This organization is a support system for incarcerated people run by people who have been formerly incarcerated and engage in community efforts such as their Heroes in the Hood program to help inspire meaningful goals within the younger generations of high-risk communities to channel their energy toward community restoration. Shepherds Fold, as a transition home, provides similar services from a faith-based approach, instilling Christian values within their participating members. One Roof, an organization whose mission is to end homelessness in Alabama, is yet another resource for people re-entering society after being incarcerated. Through their practice of Coordinated Entry, or an in-depth needs assessment, One Roof is able to secure housing for those in need and point them to additional resources they may require based on their assessment. This can be very helpful for many, especially those who have been incarcerated for decades long, and who may not be aware of what resources exist in the community, or how to go about securing them. Finally, Aid to Inmate Mothers (AIM) is an organization that provides assistance to mothers who are incarcerated, both during their incarceration, as well as their transition period into society after their sentences have been served. AIM provides transportation to children for visitations with their mothers in prison and provides incarcerated mothers opportunities to record bedtime stories for their children. Their reentry programs aim to reconnect mothers with their children, provide a few essentials for those leaving prison, provide classes on life skills, job preparedness, parenting, and other topics for those who are interested, and even provide transition housing for a year, though it comes with a few eligibility requirements, including rental fees charged weekly.
There are also educational opportunities that are provided for incarcerated people in Alabama’s prisons. The Alabama Prison Arts and Education Project led by Auburn University, and the Donaldson Lecture Series led by the University of Alabama at Birmingham (UAB) are only two such programs. The Alabama Prison Arts and Education Project provides incarcerated individuals a chance to earn college credits while serving time. These courses are offered in the field of arts and sciences, and for those who can keep up with the standards of Auburn’s academic programs, this is a great opportunity for incarcerated individuals to pursue higher education, and as a result, be better equipped to handle the professional world upon their release. Similarly, UAB also offers lecture series at Donaldson Prison. While not as extensive or academically progressive as Auburn’s program, the Donaldson Lecture Series focuses on educational talks given to incarcerated individuals within the prison every other Tuesday for academic enrichment purposes.
Shifting the Mindset Around Crime and Punishment
An image of solidarity in favor of Prisoner Rights; Source: Yahoo Images Public Domain via Racism.org
These resources are well-intentioned and have helped save so many lives to date. Yet, this is not enough; there is a much-needed shift in the societal mindset around crime and punishment. The issue of the prison system is rooted in the racist founding of this nation, and as such, has systemic implications on various areas of a person’s life. Reforms can only go so far, as they are still pieces of legislation that try to make changes to the existing laws, but they still operate under those same laws. There needs to be a shift in the way incarcerated people are viewed within the larger society, and there needs to be a reexamination of the laws on the books since most of the institutions in America are rooted in beliefs of supremacy. Some things that can help us rethink the way we approach topics that involve imprisoned people are suggested below.
As explained earlier, changing the language around how people in prison are talked about can humanize the population and foster compassion towards the group. Refer to them as imprisoned persons or people in prison rather than branding them the title of “prisoner” or “inmate”. This helps shift the narrative. “Prisoner” or “Inmate” seems to imply that these individuals are criminals at the core, and brands them as “others” in the eyes of society. Instead, referring to them as “imprisoned people” implies they are human, with natural rights, and only living in a condition of imprisonment rather than being defined by their conditions.
Finally, I leave you with a challenge: rethink how crime and punishment are framed in our society. Who is held accountable? Who isn’t? What acts are considered criminal and what aren’t? Who decides which acts to define as criminal and which ones do not? Who benefits from the current criminal “justice” system? Does committing a crime make you a bad person, a “criminal” for the rest of your life, or should you be given another chance to reform? Should people be branded innately “criminal” or are their actions influenced by the conditions of the society they live in and dependent on the context and motivations behind the crime committed? Is it fair to punish someone based on actions (mistakes yes, but still actions) committed as young people for the rest of their lives? Why is it that our society places the label “criminals” on people who commit crimes, but refuses to see them as anything else? People can be “criminals” and still be artists, musicians, poets, writers, activists, metal workers, etc. Why does our society insist on placing a singular label on this population? Could it be to easily forget their existence, to remove humanity from their essence? All these are necessary questions to ask ourselves to understand our own biases towards imprisoned people and began to rethink our own actions that can have long-lasting consequences on the lives of so many. After all, this prison crisis is happening in our own backyard, and if we do not speak out against these atrocities, we are just as guilty as those committing them.
Source: Free Alabama Movement through Yahoo Images; An image of an inmate wearing a uniform with the inscription, “Alabama Dept. of Corrections.”
WBHM, the publicly sponsored NPR affiliate located in Birmingham, Alabama, published a podcast this year, focusing on the atrocious realities of prisons in Alabama. Titled, “Deliberate Indifference,” the host, Mary Scott Hodgin, takes the listeners through an in-depth journey of the correctional facilities in Alabama, trying to better understand the root causes of the realities the people behind bars face on a daily basis. A health and science writer for the WBHM since 2018, Mary Scott Hodgin has been researching this crisis that Alabama prisons have been facing since 2019. The resulting masterpiece is her podcast, “Deliberate Indifference.”
This blog will highlight some of the themes the limited series focused on, and because this topic is very nuanced, I would not be able to do justice to this discussion in one blog. Hence, this will be a two-part series, where the first part focuses on the background of the prison system as a whole, and the historical context of Alabama’s prison system. The second part will focus on the human rights violations happening in Alabama’s prisons today, including the human rights violations existing in Alabama’s prisons today and the past, and how one can ensure that prisoners are treated with dignity and respect.
I strongly recommend that you please check out the podcast if you have not already because there are many details that I may not be able to get to in this blog or the next one that is worth knowing about. After all, this story is one close to home, and the first step towards finding a solution is having knowledge of the problem at hand. With that being said, let us dive in.
The Origins of the Prison Systems in the Southern States of America
Alabama prisons are recently under federal investigation for the increased violence and sexual assaults that have been rampant for years. This is not the first time the state’s penal system has been under investigation by the federal government. In 2017, Alabama prisons were under federal investigation for the inadequate mental health care offered to the inmates. Before focusing on the details of the prison system, some background information is necessary to fully comprehend how the system got to the place they are in right now. In the podcast, after interviewing various experts on the subject, Hodgin speaks at length about the history of prisons in Alabama. In the 1970s, following a class action lawsuit on the conditions of the prisons in Alabama, Frank Johnson, a federal judge ruled a federal takeover of the Alabama prison system until conditions improved.
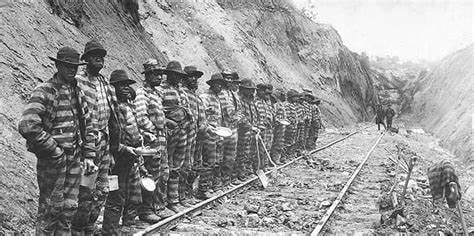
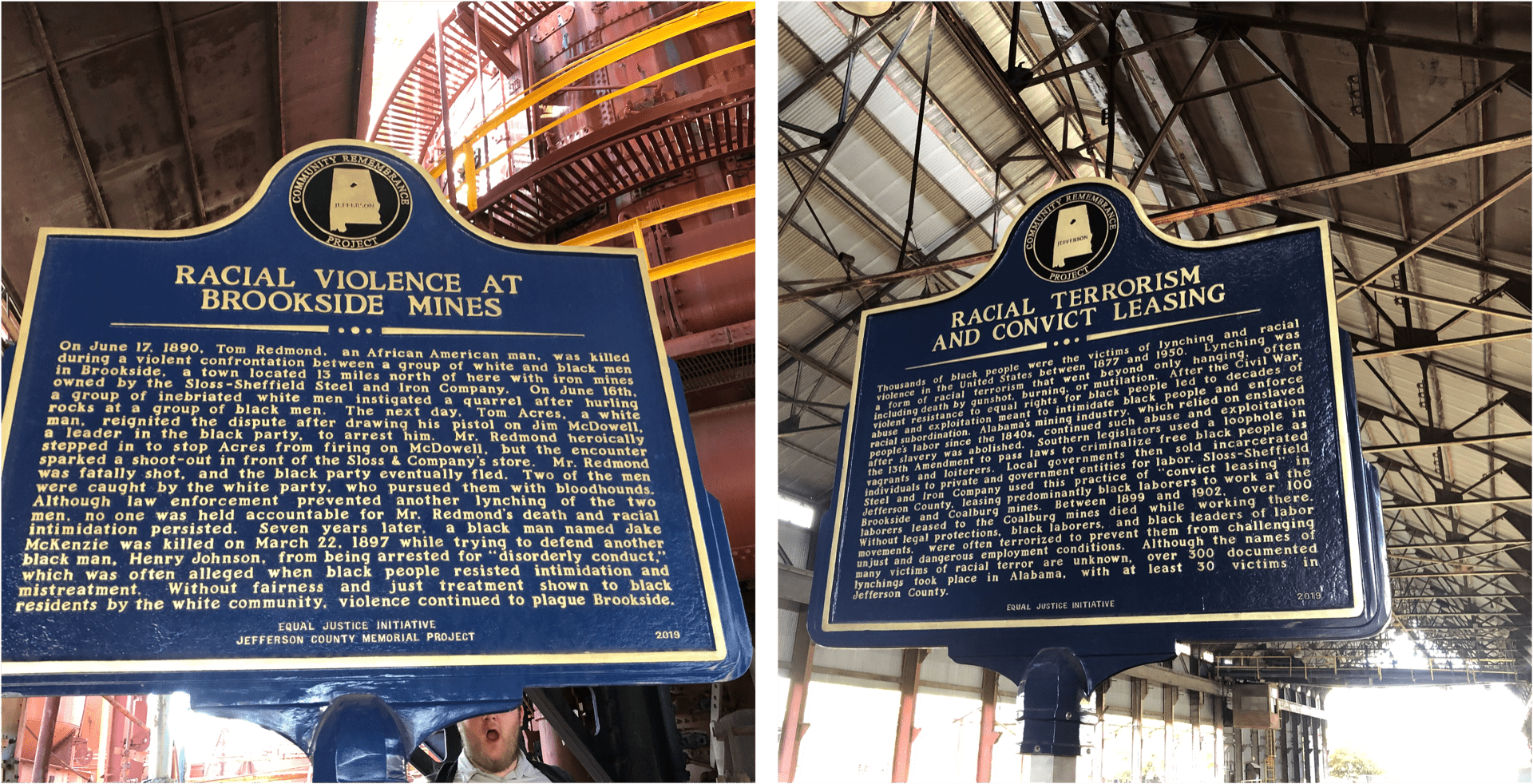
Source: Yahoo Images; An image of what the convict leasing system looked like. Prisoners worked day and night on railroads, coal mines, farms, and other places.
As reported in “Deliberate Indifference”, Wayne Flint, a retired Auburn history professor insists that the history of Alabama’s prison system goes further back, starting with the Antebellum era. Flint observes that there were two cultures during that era in the South–a frontier culture and a plantation culture. The frontier culture was only available for people considered “white,” and settlements were disputed with violence. The plantation culture, which was mostly meant for African Americans (who were set free after centuries of slavery following the Union’s victory in the Civil War), focused on the question, “How do you control freedmen?” This was made possible by the loophole included in the 13th Amendment to the Constitution, which outlawed slavery with the exception of imprisoned populations. This meant that new laws …
New laws were created, targeting African Americans, making it possible to arrest and imprison them. These new laws, known as the Black Codes, were obnoxious, to put it kindly, and very racially inspired. The Black Codes included broad vagrancy laws, meaning that any person caught unemployed, begging, or unhoused (to name a few) would be put into prison.
Of course, though there were many white people dealing with poverty at the time, the only ones imprisoned for this were African Americans. Additionally, during the Reconstruction Era, following the defeat of the Confederacy, the Southern states were struggling to rebuild their society and economy. They required cheap labor, and people willing to work long, grueling hours. All this was true at a time when Southerners were not ready to integrate with the then newly freed African Americans and did not want them to have any political power to fight the oppressive conditions they dealt with. Before the Civil War, Flint points out that the majority of people imprisoned, (99%), were White; after the war, Alabama’s prison population was made up mostly of African Americans, (90%).
The Private Sector Benefits from the Prison System
Sources: Kala Bhattar; Sloss Furnaces, the steel company in Birmingham, Alabama, has even acknowledged the company’s history of using convict leasing.
One proposed “solution” to this supposed issue was the convict leasing system. African Americans were arrested for petty crimes, placed in prison, and forced to work with little to no compensation. Due to their incarceration, the inmates’ official records denied them the right to vote. This meant that not only did these states plunge the freed people back into a form of slavery, but they also managed to take away their political power, even after they had served time. Alabama was a state that indulged in this practice. The state did not want to raise taxes, but housing incarcerated people cost the state money. Their solution was to lend prisoners to private companies which paid the state to use the prisoners’ labor; the companies did not pay the prisoners, though, in any form of compensation.
This system became extremely profitable, especially during the Industrial Revolution, which required physical labor. This is how the mining town of Brookside, Alabama grew, and this is the system employed at the famous steel company, Sloss Furnaces in Birmingham. The conditions in which they worked were atrocious during the day, and prisoners were chained to the beds they slept in at night. This system required them to work many days underground with no protection and very little sustenance. Although there were both Black and White prisoners leased under this system, the Black prisoners were treated far worse than their White counterparts. Both Black and White prisoners, if they refused to work, would be beaten, abused, refused access to basic needs, and even could be denied parole. Prisoners were violently abused for any wrongdoings and because much of the public had no knowledge of these activities, the prisoners became an invisible population and were forgotten about.
That was until 1924 when a white prisoner by the name of James Knox was murdered by being dropped into a vat of boiling water for working too slowly. This incident took place in Birmingham, Alabama. Initially, it was reported that Knox’s death was a suicide or an accident. An investigation later revealed not only was James Knox’s death a deliberate act of punishment but also that, following his death, Knox was injected with poison to artificially indicate a suicidal or accidental death.
While this incident is certainly not the only incident that has ever occurred, nor is it the most heinous, this incident, along with other similar incidents where the victim was white, brought attention to the issue of prisoner abuse, and helped put an end to much of the convict leasing, at least leasing to private companies. Unfortunately, the use of convict leasing continued to take place in Alabama and other places even after this case was ruled, but inmates were to be used only for government projects like working on highways and working on farms and cattle ranches. One piece of good news is that in 2022, Alabama voters, along with four other states, voted to close the loophole in the 13th amendment, calling for the state to stop forcing prisoners to work for free. Many other states have shown interest in following this momentum.
The First Time Alabama’s Prisons Experienced a Federal Takeover
Source: Wikipedia through Yahoo Images; An image of George Wallace, who was governor at the time of the 1970s federal investigation of conditions at Alabama’s prisons.
In the 1970s, lawsuits were filed against the state of Alabama, the State Department of Corrections, and the governor at the time, George Wallace. Upon further examination of the prisons’ conditions in Alabama, the courts ruled that Alabama prisons were functioning under inhumane conditions and authorized the federal government to step in to address the issues they found in the prisons. There was extreme violence and human rights abuses, and Judge Johnson declared that if Alabama prisons did not comply with his rulings, he would have several of the prisons closed.
Judge Johnson argued that “A state is not at liberty to afford its citizens only those constitutional rights which fit comfortably within its budget.” Judge Johnson provided details on what was expected to change, including improvements in educational opportunities, employment opportunities (with pay), better medical care, sufficient meals, and more space for each imprisoned individual. Governor Wallace, however, denied that there was any problem with Alabama’s prison systems, argued that the involvement of the federal government was an overreach that jeopardized states’ rights, and insisted that this approach by the federal government was disrespectful to the victims of crimes. Unfortunately, Judge Johnson did not see the case to the end; he accepted a higher position, passing on his work to his successor, and in 1988, the federal government ended its oversight of the Alabama prisons.
An unsettling reality becomes clear when comparing the most recent findings and the findings outlined by Judge Johnson – both reports are unnervingly similar, meaning that not much has changed since then. In fact, the issues outlined by Judge Johnson in the 1970s have only exacerbated as the prison population continues to grow, both in Alabama and in America as a whole.
The Racialized Prison System and Its Impacts
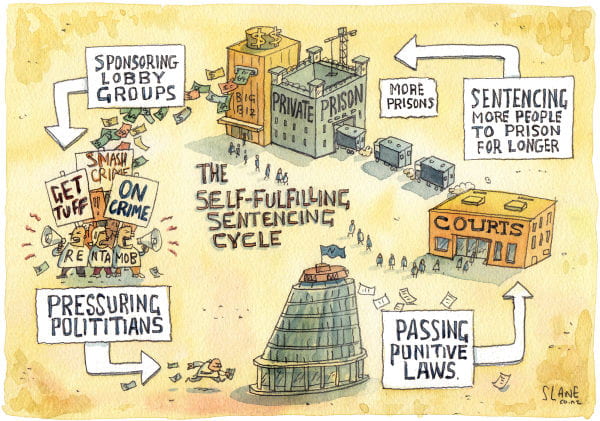
Source: Yahoo Images; The image is titled, “The Self-Fulfilling Sentencing Cycle”, between lobby groups, politicians, the justice system, and prisons.
The main issue that Hodgin consistently points out in reference to Alabama’s prisons is the overcrowding of prisoners. This issue leads to an entire range of other issues within the prison system, which will be discussed at length in the next blog. For now, the focus is primarily on how this overcrowding issue emerged in the first place.
Richard Nixon introduced his idea to wage a “War on Drugs” during the 1970s, with the intention of imprisonment for addicts rather than medical attention and/or treatment. His war had intended targets from the beginning. In an interview conducted years later, Nixon’s own aide stated that their real targets were the leftists who were against the Vietnam War and African Americans in general, but blatantly targeting them would have been constitutionally impossible. Therefore, the War on Drugs was a way for Nixon’s administration to associate marijuana with the leftist “hippies” and heroine with African Americans to disrupt their communities and arrest their leaders. Even though both the white population and black and brown populations used similar amounts of drugs, black and brown communities were disproportionately targeted and imprisoned. Hence, the unequal War on Drugs was implemented, driving up the number of people incarcerated for nonviolent crimes like possessing marijuana and heroin. This contributed massively to the increase in prison populations nationwide, including in Alabama, and this practice has continued to exist to this day, over fifty years since its implementation.
Additionally, while waging his War on Drugs, Nixon also insisted that we must be “Tough on Crimes” in order to justify his war. This approach called for longer sentencing, (even for nonviolent crimes), harsher punishments, mandatory minimums set for certain crimes, and three-strikes rules, all in an attempt to lower crime rates in the nation. The mandatory minimums set mandatory sentencing years for certain crimes, such as drug possession, giving the judges less flexibility to sentence on a case-by-case basis. The three-strikes law, or the habitual felony offender act, (the one in Alabama was passed in 1977 but other states have similar laws in place), sentenced a person to life in prison without parole after their third offense, whether their offenses are violent or nonviolent. The War on Drugs, the tough-on-crime initiative, and the various sentencing laws that followed this era exacerbated the overcrowding of prison populations, including in Alabama.
Nixon’s successor, Ronald Reagan continued Nixon’s War on Drugs, and his wife, Nancy Reagan, started the DARE campaign to teach students across the nation to “Say No to Drugs.” In an attempt to fearmonger the public to support the war on drugs and the tougher sentencing laws, the media played a big role in framing the issue of crime to be a result of increased drug use, a misleading fact that has yet to be proven. In fact, many studies today show that wherever there are high levels of poverty, there will also be an increase in crime rates.
With all this being said, there has been a growing movement in Alabama from both the Republicans and Democrats, to repeal the Habitual Felony Offender Act, citing the overcrowding issues and sentencing that doesn’t fit the crime. The House Judiciary Committee of Alabama approved this repeal in 2021, and the legislation was set to be voted on by the full House. After much research and various combinations of google searches, I found out that the repeal was halted on April 7th of 2022, labeled “dead/failed/vetoed” on the bill tracker website. While this is not the best news, by spreading more awareness of the impact this single piece of legislation has had on many lives in the state, there is hope that with increased support, it may pass in the future. However, this alone will not be enough to address the issues facing Alabama prisons.
In the upcoming blog, we will focus on the prison conditions, details of the 2017 reports and 2020 reports, how the pandemic has exacerbated these issues, and some ways to move forward. In the meantime, listen to “Deliberate Indifference” by Mary Scott Hodgin, and stay tuned for the next part of this series.
With the increase in world crises, others become forgotten. Seven years and the Yemen Crisis is still one of the worst humanitarian crises in the world. Unnoticed, unseen, and unheard, the cry for help from the suffering in Yemen has been largely forgotten. Yemen has always been the most vulnerable country in the Middle East, even prior to the 2015 Civil War. With the worst rates of malnutrition, more than half of the Yemeni population has been living in poverty with limited to no access to resources need to live. With such an important, detrimentally impactful crisis, why has there been silence surrounding solutions?
Source: Yahoo Images
Why is there a Crisis?
The Yemen Crisis began with a civil war between the government forces and the Houthis, also known as Ansar Allah. In the past seven years, the residue of the civil war in Yemen continues to worsen tremendously. The conflict has been between the internationally recognized government, backed by the Saudi government, and the Houthi rebels backed by Iran. The war was caused by many factors. Given that Yemen was already one of the poorest Arab countries, any change would cause a political division. These factors include fuel price increasing, the Houthi rebels taking over and causing a military division, and the involvement of Saudi Arabia. Many countries have gotten involved – not to solve the crisis, but to pick the side supporting its agendas and send military equipment and personnel in support of these goals. This has left civilians in grave danger.
Source: Yahoo Images
Conditions of the Crisis
The country’s humanitarian crisis is said to be among the worst in the world, due to widespread hunger, disease, and attacks on civilians. There have been around 6 million individuals displaced from their homes since the beginning of the catastrophe. There are 4.3 million civilians internally displaced. As of 2021, Yemen had one of the largest numbers of internally displaced people (IDP) in the world. Many IDPs have been living in a constant state of fear and suffering. Being in a state of exile, having insufficient environmental and living conditions, they have no access to the resources needed to survive day to day. In addition, food insecurity, lack of clean water, healthcare, and sanitation services have caused tremendous issues for countless of civilians still living in Yemen.
Women and Children
In the heart of the crisis, the most affected have been found to be women and children. With the state of the country, inflation, along with scarcity of economic opportunities, many families can no longer afford basic meals, leading to high cases of starvation. Further, many cases of gender-based violence, exploitation, and early marriage are on the rise. Malnutrition rates for women and children in Yemen are the highest in the world. About 1.3 million breastfeeding and pregnant mothers are in need of treatment for malnutrition. There have also been found problems with children being forced to fight in the war. In 2019, there were 1,940 children fighting as soldiers.
Source: Yahoo Images
Mental Health
Mental health in Yemen has deteriorated over the causes and outcomes of the conflict. Individuals have dealt with losing family members and friends, their homes, suffering from displacement, violence due to war, food insecurity, unemployment, diseases, torture…the list can go on and on. With all these factors causing grief then leading to long term depression, individuals in Yemen are not able to seek the proper resources needed. There are about 30 million people living in Yemen in 2020 but only 59 psychiatrists. Meaning, for every half a million, there was only one psychiatrist. With the mental health stigmas already a huge concern in the Middle East, many individuals either do not know they need mental health services or are not allowed to seek them. For instance, women have to ask for permission from their families, particularly their husbands, in order to seek mental health services.
What is the World doing?
The United Nations (UN) has backed and presented peace negotiations, but it has only seen limited progression. The UN found that regional actors involved in the conflict have played a strong role in slowing down the peace process. Observers of the crisis see that the involvement of Iran, Saudi Arabia, and the UAE, have prolonged the war and worsened its conditions. The response of the world needs to strengthen when dealing with the Yemen crisis. As we have seen support from the world given to the Ukrainian crisis and the crisis in Afghanistan, as a whole, a change is possible. The most important thing we can do is talk about the crisis. This has gone unheard, but with a collective voice we can urge and find a solution.
Source: Yahoo Images
What can you do?
The best thing you can do regarding the Yemen crisis is to educate yourself, engage in conversations, and make others aware of what is happening. Below are a list of books and sources to keep you updated in ways you can help.
Note from the author: This blog was written to accompany the social justice cafe on Wednesday, November 30th at 4:00 pm on zoom. To join, sign up here. Alongside this event, this post focuses on an international scale while the recent post by Maya Crocker focuses on transitional justice in the United States.
Forgiving and being reconciled to our enemies or our loved ones are not about pretending that things are other than they are. It is not about patting one another on the back and turning a blind eye to the wrong. True reconciliation exposes the awfulness, the abuse, the hurt, the truth. It could even sometimes make things worse. It is a risky undertaking but in the end, it is worthwhile, because, in the end, only an honest confrontation with reality can bring real healing. Superficial reconciliation can bring only superficial healing.
Archbishop Desmond Tutu
Figure 1: Source: Flickr, John Mathew Smith; Archbishop Desmond Tutu in Washington, D.C., 1999.
What is transitional justice?
Transitional justice (TJ) refers to a set of judicial and non-judicial processes addressing previous injustices of authoritarian regimes (or multiple perpetrator groups) and establishing rule of law. Transitional justice has several aims and synthesizes aspects of punitive and restorative justice.
According to the United Nations Office of the High Commissioner on Human Rights (OHCHR), these aims include:
Providing recognition to victims
Building trust between citizens and state institutions
Reinforcing the rule of law
Committing to human rights and building solidarity with victims
Reconciliation between victims, perpetrators, and bystanders
Preventing new violations
But only characterizing transitional justice through its aims would not highlight the transformative effect this approach attempts in states where massive or systematic violations have occurred. While providing redress to victims and undertaking prosecutorial avenues as practical solutions, this approach also takes a strategic initiative to change the political systems, conflicts, and conditions that contributed to violations occurring in the first place.
This field first emerged in the 1980s and early 90s in response to the drastic political changes in Latin America and East Europe. Human rights advocates and citizens alike questioned how and what kind of redress should occur in the wake of widespread and systematic violence. Fears over disrupting political changes by pursuing indictments of former leaders were salient: how could justice exist without compromising democratization?
Thus, “transitions to democracy” and “justice” intersected and involved multiple processes to be sensitive to these concerns during a critical period in the country.
Truth Commissions: ad hoc commissions of inquiry established in, and authorized by, states for the primary purposes of investigating and reporting on key periods of recent past abuse.
Amnesty: a pardon granted to perpetrators, usually granted to those who comply with truth commissions and offer testimonies
Purges, lustrations, and security reforms: (1) removal of known collaborators of oppression from office and state institutions, (2) process of vetting personnel in state institutions, (3) transformation in state institutions involved in repression, like the military, police, judiciary
Reparations: state-sponsored initiatives that aim at repairing, on a massive scale, the consequences of past abuse experienced by certain classes of victims, including material and symbolic benefits
Gender Justice: focusing on the intersections of human rights abuse and gender during a period of repression, fact-finding initiatives to establish the nature of gendered abuses
Memorialization: museums, memorials, and other means of preserving the public memory of victims and raising moral consciousness about past abuse
Ultimately, TJ is a context-specific process that crucially (and historically) is led by the nation where the violations happened.
Specific attempts at transitional justice: the good and bad
Bolivia:
Days after the restoration to democracy in 1982, the government created the National Commission of Inquiry into Disappearances. No reports or prosecutions were produced. In 1986, prosecutions began against the former military leader, General García Meza, and some of his officers. The trial was not complete until 1993, by which point Meza had gone into hiding to avoid a 30-year sentence for torture and murder. Notably, this court case rejected pardons for those convicted of crimes against humanity.
Uruguay:
After a 12-year military rule in 1985, the new government avoided truth commissions. Instead, President Sanguinetti issued a pardon (1986) to all soldiers and officers of the previous regime, with no distinction as to those who followed orders and those who gave them. He claimed this was the ‘safest path’ but ‘not a moral decision,’ highlighting that TJ attempts are not pursued in every situation. This is often a result of corruption and officials often rely on a dialogue of ‘national reconciliation by granting large amnesties but failing to pursue any other TJ processes, essentially dismissing victims’ realities. Victims were denied any form of reparation and violators remain in high office in the police and military. An official Commission for Peace was established in 2000 under President Jorge Batlle with the official report released in April 2003 confirming that the military dictatorship was involved in some of the disappearances.
Chile:
This history of Chile’s dictatorship and eventual prosecutorial redress can be read about in my next blog. Part of the reason for the near-decade gap between the restoration of democracy (1990) and Pinochet’s arrest (1998) was due to Pinochet’s change of the constitution during military rule. Not only did he pardon himself and his torturers in 1978, but he enshrined legal protections from purges and lustration attempts. Nonetheless, Chile has engaged in memorialization and reparations in the cases of successful prosecution of former DINA police.
El Salvador:
A Commission on the Truth of El Salvador was established in 1991, led by three international jurists and staffed and financed by the United Nations. While only fully investigating 33 disappearances out of the reported 22,000, the commission did identify 40 individuals connected to the armed forces and involved in crimes against humanity. Additionally, the Commission was able to confirm the El Mozote massacre, where nearly 1,000 villagers were killed by US-trained and equipped Salvadoran army members. The Commission also called on the Supreme Court to retire, which they declined. René Ponce was named general and ordered the execution of 6 Jesuit priests (one the then head of the Human Rights Institute). Due to Ponce’s involvement in the peace negotiations and settlement with FMLN, his prosecution was never attempted. The report from the truth commission was rejected and the then-president offered a blanket amnesty for all political crimes which the Supreme Court upheld (1995). After 20 years, no other transitional justice attempts have been implemented.
Haiti:
Haiti suffered massive human rights violations under the Duvalier reign between 1957 to 1986. Over 40,000 Haitians were killed and it wasn’t until 1990 that democracy was established with the election of President Jean-Bertrand Aristide. Soon after, he was ousted by General Raoul Cedras, showing just how volatile transitions toward democracy can be. Under Cedras, hundreds were killed by the paramilitary group Front for the Advancement and Progress of Haiti (FRAPH), funded in part by the CIA. Democracy was restored in 1994 and power returned to Aristide but at the cost of blanket amnesty for all rapes, murders, and political killings. He went on to establish a National Commission for Truth and Justice which in February 1996 urged for the prosecution of individuals who committed crimes against humanity by an international tribunal. There has been no tribunal and no prosecutions, and to this day impunity is chronic.
Argentina:
Figure 2: Source: Yahoo Images, Colin Snider; Graffiti of General Jorge Videla with the phrases “More than 30,000 reasons for popular justice. Never again look the other way.”
Argentina took the most extensive approach of the states discussed so far. In 1983 after the defeat of the military in the Falklands Wars, President Raoul Alfonsín annulled the amnesty the military had given themselves. He also set up the Commission on the Disappeared which produced the report Nunca Más (Never Again) which was a national bestseller – fulfilling some forms of memorialization. The evidence the commission gathered was used to prosecute 5 of the most senior members of the military junta, but when indictments began on less senior officers the military revolted in 1987. Trials ceased to end the conflict but Alfonsín refused to give any pardons. His successor Carlos Menem was the one to pardon ex-president Videla and others on grounds of “national reconciliation.” In spite of Menem’s undermining, human rights groups and families of the disappeared renewed the vigor for criminal accountability in 2003, and as of 2010, more than 800 face criminal charges and 200 have been sentenced.
South Africa:
When one thinks of “truth and reconciliation” or “truth commissions,” the most likely example to come to mind is South Africa. After the end of apartheid (a crime against humanity) in 1994, the new democratic government formed the unique tripartite Truth and Reconciliation Commission (TRC). It had three responsibilities: (1) record the apartheid era for memory, (2) make recommendations for reparations, and (3) grant amnesty to individuals based on application and only in limited circumstances.
This was a revolutionary step for transitional justice and helped citizens come to terms with the violent and discriminatory apartheid. In spite of the success of this TRC, no prosecutions have ever been mounted and organizations like Human Rights Watch and Amnesty International fear the TRC suggestions are not being fully implemented.
Nonetheless, it is important to note that the commission was chaired by none other than Archbishop Desmond Tutu whose ceaseless human rights efforts have helped define the role of TRCs as both forward and backward-looking. In his words, “True reconciliation is never cheap, for it is based on forgiveness which is costly. Forgiveness in turn depends on repentance, which has to be based on an acknowledgment of what was done wrong, and therefore on disclosure of the truth. You cannot forgive what you do not know.”
United States:
For an in-depth examination of the transitional justice movement in the United States, please read Maya Crocker’s blog here.
Conclusion
Without addressing the seeds which sprouted violence, the threat of their reoccurrence cannot be escaped. This means acknowledgment, and hardest of all, forgiveness. While a generation suffered, hatred should not be allowed to pass down and threaten long-lasting peace.
This is not easy, but if you believe in human rights, affirming the realities of victims and perpetrators and all those in between is crucial. As Desmond Tutu says, “We must not only speak about forgiveness and reconciliation, we must act on these principles.”
This post draws a lot of information from the book Crimes Against Humanity: The Struggle for Global Justice by Geoffrey Robertson, originally published in 1999 with multiple editions given the continuous development of human rights. I will be utilizing information from a 1999 edition, and thus, certain information on the results of transitional justice attempts will have developed more in the last two decades. If you are interested in obtaining a copy for yourself, the latest edition was updated in 2013 and includes additional sections on Iraq, Guantanamo, the Obama administration’s use of drone warfare, the Charles Taylor conviction, and the trials of Mladic, Karadzic, and Khalid Sheik Mohammed.
Figure 3: Source: Target; Cover of the aforementioned book.
Geoffery Robertson is an internationally acclaimed lawyer and human rights advocate who has served as a UN war crimes judge and founded Doughty Street Chambers in London, a leading human rights law practice. In his book, he deconstructs international human rights law, beginning with the foundational philosophy of rights dialogue (natural rights, social contract, Enlightenment) and moving through the defining events of 20th-century human rights law formation. His book is written in a non-legalese, prose-like style and is a strong starting point for learning a breadth of information about the very complex processes behind prosecutions (and more often why they don’t happen).
If this interests you, read Robertson’s book or check out more blogs from IHR below:
What is the International Criminal Court and Why Should I Care?
“Statue of Lady Justice” Source: Jernej Furman via Flickr
Note from the Author: This blog was written to accompany the Social Justice Café Transitional Justice: Here & Now hosted by the Institute for Human Rights at UAB on Wednesday, November 30th at 4:00pm CST. At this event we will discuss a brief history of Transitional Justice in the United States and hold an open discussion about what it could look like in the home city of the Institute, Birmingham Alabama. You can find out more information and join the virtual event here. In this post, we will explore transitional justice in the United States. We will have another post on the international context of transitional justice.
Transitional justice is a field of international justice that “aims to provide recognition to victims, enhance the trust of individuals in State institutions, reinforce respect for human rights and promote the rule of law, as a step towards reconciliation and the prevention of new violations” (OHCHR). Often referred to as TJ, transitional justice is a system of multiple mechanisms and processes that attempt to create stability and ensure justice and remedies for victims of oppression and human rights transgressions. Some of the most commonly used mechanisms of TJ are truth commissions (TCs), reparations, and trials of perpetrators.
In practice, transitional justice has often been restricted to nations following active conflict or repressive authoritarian regimes, otherwise known as transitional time periods. This traditional understanding of transitional justice is beginning to evolve as stable, established democracies like Canada and South Korea implement TJ mechanisms such as truth commissions and reparations to address and amend state-sponsored abuses of certain groups. As it evolves the international gaze has once again turned to the United States and the uncomfortable discussion about the historical and ongoing oppressions. This article intends to establish the historical basis of transitional justice in the United States and recent developments to encourage a conversation about acknowledgement, fact-finding, reparations, and justice in the land of the free.
Section 1: Historical Examples of Transitional Justice in the United States
With an international spotlight on the Black Lives Matter movement in the United States in 2020 came an increase in conversations about reparations to African Americans for the abuses of slavery, segregation, police brutality, prison labor, exclusion from housing and education and other forms of state-sponsored oppression that have proliferated for centuries. The discussion about the harms the American government has caused to Indigenous tribes, Alaskan Natives and people of Hawai’i, and other marginalized groups has been a matter of public discourse for decades. While the word reparations saturated international media, little attention was given to what reparations would truly look like, could look like, and examples of when the United States have provided reparations before.
While the spotlight of this discussion about reparations is often on monetary forms, such as property, cash or pensions, transitional justice recognizes that reparations can and should come in many different guises in order to provide a more holistic and healing process for victims. Reparations are deeply context-specific, and should be tailored to the needs of the victim, nation, and individual circumstance. However, examples of other forms of reparations and TJ include official acknowledgements and apologies, funding of research to uncover facts and educate the public on the truth, providing education and/or healthcare to victims and their families, and preserving historical sights and monuments. Ultimately, they should be determined by and catered to the people involved.
I have included both a brief infographic timeline and a more detailed look at a few examples of government-led transitional justice mechanisms in the United States below. It is important to note that, as many of these instances occurred prior to our modern definitions of transitional justice and reparations, this timeline encompasses cases of compensation which, under similar circumstances today, would likely be considered reparations, but were not explicitly intended as such at the time. The same goes for fact finding commissions that are analogous modern Truth and Reconciliation Commissions, though they lack that title. I have excluded instances of payments or acknowledgements being issued following a lawsuit through our judicial system, as well as instances of TJ being led by non-governmental entities like community organizations, charities or other non-governmental institutions.
Infographic by Maya Crocker for the Institute of Human Rights. Source: https://guides.library.umass.edu/reparations
President Lyndon B. Johnson established the National Advisory Commission on Civil Disorders, otherwise known as the Kerner Commission, in 1967. It was established to serve the purpose of a fact-finding mechanism akin to a Truth Commission today. The goal of the commission was to identify the causes of the violent race riots of 1967. While widely ignored, the Kerner Commission found that the root of the unrest were unequal economic opportunities, racism, and police brutality against minority racial groups in America.
Following concentrated efforts from interest groups and international attention, the United States federal government committed to two massive examples of explicit transitional justice mechanisms in the 1980s for Japanese Americans that were interned by Executive Order 9066 during World War II. In 1980 President Jimmy Carter signed the Commission on Wartime Relocation and Internment of Civilians (CWRIC) into law, establishing a clear transitional justice mechanism (truth commission) at the national level. The CWRIC published the full report of their findings in February of 1983, and momentum from the commission persisted with the recommendations which were published in June 1983. The recommendations included an official apology, pardons for those convicted of violations of the executive order or during detainment, and the establishment of a federally funded foundation for research and education on the incident.
Shortly after the results of the CWRIC circulated across the nation, the United States Congress passed the Civil Liberties Act of 1988 which provided all eligible interned individuals with a one time payment of $20,000 in reparations as well as official acknowledgement and apology from the United States. In addition, all individuals who were convicted of disobeying the executive order or violating rules while interned were officially pardoned.
In response to the massive Black Lives Matter protests in 2020, many subnational level truth commissions and reparations programs were initiated, including those in the State of California, Evanston, Illinois, and Asheville, North Carolina. As the national conversation continues, we may see an increase of examples of transitional justice at work in United States communities.
“Freedom?” Source: Nicu Buculei via Flickr
Section 2: You, us, and the future of transitional justice in the United States
Whether in Europe, Africa, the Asia-Pacific, the Middle East, or the Americas, civil society plays a key role in the transitional justice sphere. Civil society actors are civilian organizations which can be activist groups, media, charities, non-profit organizations, educational groups and schools, or just citizens interacting with policy. Most recent transitional justice measures that have been implemented in the past few years in the United States have been on the subnational level. They are occurring as a result of citizens’ calls for action, constant attention on the need for transitional justice, and the everyday acts of discussing transitional justice.
Birmingham, Alabama is a historic city for human rights, civil rights and civic action. Civil society here, in this city, has influenced national change through the Civil Rights Movement as well as citywide changes like the removal of confederate statues in public parks and the preservation of historic sites from the Civil Rights Movement like the Greyhound Bus Station and 16th Street Baptist Church.
The Institute of Human Rights at UAB fosters an educational environment where you can see civil society at work, and hosts Social Justice Cafes on the second Wednesday of every month during the school year at 4:00pm CST. We will be hosting our last Social Justice Café of the semester, Transitional Justice: Here & Nowon Wednesday, November 30th to discuss what transitional justice should look like in American cities like Birmingham. You can find out how to join these open discussions, and become a civil society actor yourself, and attend more free educational events from the Institute of Human Rightshere.
Cameroon, once a bastion of peace and tranquility, is now a nation beset with a series of violent and armed conflicts. Since late 2016, an armed conflict between the state defense forces of Cameroon and the non-state armed groups (NSAGs) of Southern Cameroons’ has ravaged the country. In the last six years, there have been more than 6,000 deaths, 765,000 internally displaced persons (IDPs), and 70,000 registered refugees in neighboring Nigeria, with approximately 2.2 million people in need of humanitarian aid. The Norwegian Refugee Council has referred to the conflict as one of the most neglected in the world. The long-term human capital consequences of this conflict are enormous.
A more comprehensive background of the armed conflict and humanitarian crisis in Southern Cameroons can be found in a previous IHR blog post, “Cameroon, a Nation Divided”.
Source: via Yahoo Images
It is against this backdrop that the Cameroon Humanitarian Relief Initiative (CHRI) in partnership with the Institute of Human Rights (IHR) co-hosted an international webinar, “Updates on the Humanitarian Crisis from the Ongoing Armed Conflict in the Southern Cameroons”on the 18th of October, 2022. The aim of this event was to discuss the current humanitarian crisis from a multi-perspective panel. The speaker biographies can be found at the bottom of this blog post.
Excerpts from this webinar were edited and woven together for this blog post. The full recording of the webinar is available on request by contacting ihr@uab.edu.
Source: via Yahoo Images
Overview
What are the current humanitarian needs for Internally Displaced Persons (IDPs) in Southern Cameroons?
Atim Evenye: The current context and the magnitude of the ongoing crisis in the Northwest and Southwest regions remain tense. There is continuous violence in targeted areas. We have the destruction of properties. We have abductions and kidnappings of both community people and administrators. We have killings and local arrests. We have continuous attacks on schools and students. Humanitarians face threats and direct [armed] attacks. [These are carried out] by both parties, the non-state actors and the state defense forces.
The population [has] really [been] under duress and stress for over six years.
Food Security: Atim Evenye: When it comes to the current needs for IDPs, at the moment, I would say food security remains one of those outstanding needs. Especially in the rural areas, because these IDPs have fled their place of abort. They don’t have access to their farms. [As such,] they don’t have the economic capital [for even] daily subsistence. So, there is a lot of dependencies now on family members, [or] world food programs, and other humanitarian organizations bringing food assistance in the area.
Education Accessibility: Atim Evenye: There is a strict restriction around education. In [the rural areas] of the Northwest and Southwest regions, we have children who have not been able to go to school until date. In urban areas, there is a possibility of schools for those who can afford it. Currently, in our zone in the Northwest and Southwest regions, we have lost one month [of school this term], because we are only starting now. So, it becomes challenging on how to catch up. There’s a need for accelerated learning. [Additionally,] teachers have been abducted [and] schools have been burned. [To add to that,] there is a lot of psychological trauma, [as] many children have witnessed or experienced violence firsthand. Both the state and non-state actors [are] not conscious of the impact their actions are having on children. The government doesn’t want to hear about community schools as prescribed by the separatist. So, it’s really very challenging to access education.
Dr. Emmanuel Nfor: Education is one of the issues at the origin and at the core of the crisis, and formal education has been used by NSAGs, [the non-state armed groups], as a political instrument. NSAGs have advocated and enforced a “no school policy”, leading to public school closures for the past four years in many areas. More than fifty percent of threats against buildings in communities have been directed against schools, and many school buildings have been taken over by organized armed groups. Accessing education in emergency services, or going to school in such a volatile environment, is proven to be risky for children, as well as for teachers. Pupils who were in school in most rural areas have dropped out, some joining armed groups, others displaced, and some have outgrown their ages for the classes in which they were and cannot continue. Many parents have lost their means of livelihood and are unable to sponsor their children in school. Despite repeated calls from humanitarian and human rights organizations for education to be depoliticized, schools have been burnt, teachers and students intimidated, kidnapped, and even killed, and some have seen their hands chopped off by members of armed groups.
Gender-based violence (trigger warning): Atim Evenye: We see [a great deal] of gender-based violence. In certain assessments we have conducted, for example, [many of these] young girls in rural areas are not able to go to school. What are they left to do? There is a lot of harassment, rape, and [sexual assaults]. They’re looking for five hundred francs CFA, that’s like one dollar, to [be able to just buy] food to eat. So then, they depend on young men to give them that money. And at the end of the day, they [get pregnant and become] teenage mothers. The whole cycle is really detrimental, it’s a really difficult one.
Dr. Emmanuel Nfor: Sexual violence is rampant, as a direct consequence of the crisis but also due to decreasing livelihoods, negative coping mechanisms, and lack of protection structures. The boy child is an endangered species, at risk of accusation and arbitrary killing from GFs [state defense forces], and forced recruitment by the NSAGs. There are no specific programs by both UN agencies and Internal bodies that address the needs of the boys.
Housing: Dr. Emmanuel Nfor: If we look at where the IDPs in particular are, we have IDPs that are living in the rural areas, in the bushes. We have those living within host communities. We have some that have been able to rent. [But if] they are able to pay for accommodation, [there are] a lot of difficulties because they want them to pay upfront, and they cannot do it. In all three groups, they lack basic WaSH and health services, NFIs [non-food items], and protection from natural hazards. Those who fled to other regions face stigma and severe protection risks related to exploitation, and socio-economic vulnerabilities including extortion, sexual exploitation, and child labor.
Healthcare: Atim Evenye: The next principal need I would say is around healthcare. In recent times we have [had] heath centers burned, and the staff attacked. So, it’s really challenging. Statement needs to be completed, even before the crisis, access to health care has been a serious challenge, especially in rural areas. And then, currently, with the crisis, it’s even more exacerbated. It becomes difficult now [for] humanitarians on the ground who are trying to meet the needs of these people. Take, for example, Doctors Without Borders. They have [had] to put their activities on the hold because they had issues around access [and safety] of their staff.
Dr. Emmanuel Nfor: [There is a lot of] healthcare [needs] for the vulnerable. [Safe practices in regard to] water, sanitation, and hygiene are not being followed. People who live in rural areas don’t have a good source of water. But they could be educated on the fact that even though your source of water is doubtful, you could take it, you boil it, you purify it, or you do something to make it [potable]. That education, they don’t have, or the chemicals for water treatment. Additionally, there is a lack of emergency medical and psychological units, to provide emergency care to the wounded and psychosocial support to those traumatized by the violence. We can educate people on how to prevent simple infections. How can you prevent diarrhea infection? How can you prevent malaria? If this education is done, it could be [one] way to [improve basic healthcare].
Healthcare, which is supposed to be a protected area, unfortunately, has not been the case in this conflict. We have had health centers closed; more than fifty percent of the health centers in rural communities have been closed. Not only the health centers, [but] the health workers do not feel comfortable staying there. So, a lot of them have abandoned [the centers]. The [people] left in these communities cannot access healthcare. Women cannot access antenatal clinics. Vaccinations [are] not being done, and thousands of children are at risk of contracting common vaccine-preventable infections.
The population has been abandoned to themselves.
Health centers that are open in semi-urban and urban areas are overwhelmed by people who have [been forced by the conflict to flee]. And what’s worse is that most of those who have [fled] do not have the means to pay for the treatment. We have some health centers that have accumulated huge unpaid bills because those who access healthcare cannot afford to pay those bills. For the facilities that are open, IDPs cannot afford to pay for the treatment that is given to them.
We have [also] had cases of drugs and other medical equipment [being] seized along the way by organized armed groups. So, it’s difficult to render care because the drugs and medical supplies do not reach the vulnerable in the hard-to-reach areas. Free supply of drugs and medical equipment is disturbed by locked downs, roadblocks, and/ or are seized at gunpoint.
Then the last very worrying thing is that healthcare workers are being attacked or kidnapped for ransom. A lot of them have been attacked both by the non-state actors and by the state forces; [health workers are] kidnapped by the non-state actors and/or arrested by the [state forces]. So, it is not safe [from] either side. They see you as collaborating with the other, and [so the question is] whether you should treat wounded combatants or not. According to the healthcare regulation, we take any wounded persons as patients. But unfortunately, when these [combatants are] treated, we [the healthcare workers] are blamed. The non-state actors blame you for treating the state forces. The state forces blame you for treating the non-state actors. It’s really a dilemma in which we are in.
Future Directions:
Looking towards the future, are there any resolutions to the humanitarian crisis in Southern Cameroons that you can think of that can be implemented at this point?
Dr. Emmanuel Nfor: I think the first thing we need to consider for the humanitarian crisis is that we need to speak the truth.
We need to make a truthful appraisal of what is happening on the field. Address the needs. For example, we are told that the crisis in Cameroon is one of the least funded in the world. Why? Because the data and the reposting are for some reason concealed.
So, if we must be able to go forward with the humanitarian situation, we need to know how many people are living in the bushes, how many are living in host communities, in what conditions are they living, and be able to address it. [These] figures are often contested, they say the number is lower, or they want to sway the number for their gain. So, we must start with you right data. If we have the right data on needs, it will be possible to see where the solutions should come from.
Possible resolution options, specifically for the humanitarian crisis, could consider the following:
-A community-based approach to raise awareness of protection risks in the community and identify and support community-based solutions.
-Advocate for access to civil documentation, especially birth certificates, to avoid a stateless generation and mitigate protection risks associated with a lack of civil documentation.
-Support community mediation of localized conflicts to reinforce the dialogue between host communities and IDPs and avoid tensions within the communities.
-Advocate with parties to the conflict to respect the protection rights of communities, and respect International Humanitarian Laws.
-Finding durable solutions for IDPs intending to stay in their host communities, like those who have established businesses in the new areas.
-Shelter support in rural areas as a high percentage of households live in tents or informal collective shelters
Atim Evenye: When it comes to setting strategies that we can use to resolve this conflict, I would say it’s imperative, for the powers that be to consider the roles of different parties in the conflict. There is a need for parties in this conflict to come to the table and talk. There is a need for dialogue. There is a need for unity. We need to have a unity of purpose, to push our agenda in one voice.
True is the fact that they have been the major national dialogue, [there] have been consultation meetings and other forms of dialogue in smaller circles. But the question is, during this dialogue are the needs of the different parties considered?
For example, we have women who have suffered a lot as a result of this conflict. But at the same time, we have that arm of women who are also seeking solutions on how to resolve the conflict. Women are now spearheading and speaking for themselves. And I think, there is a need to give a listening ear to what the women are saying because I think time in memorial, women have always demonstrated that ability to resolve conflict. So, one way to consider the proposals that women are giving here in Cameroon.
Secondly, there is a need to give academia and research a place. There are a lot of people in the academic who are gathering data, but the fear around it is the dissemination of this information. The administrative system is such that once you do a publication that is not supportive of what is happening, you get targeted. And by both sides. Thus, we try to be balanced in all information dissemination. There is a need for that deliberation and freedom of speech, especially in the area of academia. People should not be afraid to publicize or to make public the research and the results of what they have found in the field. So that’s another way that can be an added value to the approaches to conflict resolution.
Also, there is a need to consider the root causes. The conflict did not just start like that, it degenerated along the line. So, there is a need to go back to the drawing board and understand what pushed the Southern Cameroonians to arrive at this point. What are the different trends that have been changing through the crisis?
When it comes to how to resolve the humanitarian crisis, I think the humanitarian needs are more than what the humanitarian organizations can do, funding is very limited. It’s obvious that humanitarians cannot meet all the needs. So where should we turn to? We should turn to other actors who can bring assistance. We have development actors who can bring resilient, [long-term, skills-building] projects so that the communities will not be too dependent. The people of the Northwest and Southwest have never been those who are dependent on handouts.
They are people who are hard-working. We hear the aches of people wanting to be self-sustaining. They want to just be, to go back and be what they had been doing [before the conflict].
Dr. Emmanuel Nfor: If we don’t put away falsehood, if we don’t speak the truth and have the right data and have the right information about what is going on, on the ground, we will continue for many more years doing much but with very little impact.
The people of Northwest and Southwest can lead by themselves. These are hard-working people. They just need to be empowered, to go back to where they have lived before. There are many people who are longing to go back home, but the problem is that they go to homes that have been burnt. They go to farms that have been abandoned. They go to be reminded of the horror. So, we need psychological treatment and support. We need some form of equipping them to be able to cope with what they have lost. We should be able to end the hostilities and give people the opportunity to go back home.
So, we should rather empower them, than continue to give them aid. Let peace reign, [so that] we can empower them to reveal what they have lost and then see how they can bring up that life again. [Then] we can go forward. But hostilities should cease, and we should speak the truth; to face each other face-to-face and speak the truth.
Speaker Biographies
Atim Evenye Niger-Thomas, received a Ph.D. in Student Conflict Management and Peacebuilding at the International University of Applied sciences for Development (IUASD) Sao Tome in partnership with IPD Yaoundé. Since 2016, Atim Evenye has worked and grown in different roles at the Authentique Memorial Empowerment Foundation (AMEF). Currently, she holds the position of Assistant Director and trainer for Humanitarian Negotiation. Under this supervision, AMEF has grown to be one of the leading humanitarian organizations in the Southwest Region. AMEF runs four core programs namely,Education and Child Protection (ECP), Economic Development and Livelihood (EDL), Gender, Protection and Peace (GPP), Health/Nutrition/ WASH (HNW).
Dr. Nfor Emmanuel Nfor, holds a PhD in Medical Parasitology from the University of Yaounde I, Cameroon. In February 2017, he joined the Cameroon Baptist Convention Health Services (CBCHS), as the Malaria Focal Point. While working with the CBCHS, he attended a Peer Review Workshop on Humanitarian Negotiation organized by the Centre for Competence in Humanitarian Negotiation (CCHN) Geneva. After many other online courses, and several National and International Conferences, he was appointed Trainer and Advisor of Humanitarian Projects within the CBCHS. In this capacity, he coordinated projects executed by the CBCHS with funding from WHO, UNICEF, and UNFPA. He has been at the forefront of Humanitarian activities within the CBCHS during the ongoing sociopolitical crises in the North West and South West Regions of Cameroon, working closely with the Cameroon Humanitarian Response Plan.
This is the second in a series of blog posts that will look further into the conflict in Cameroon. Each month a humanitarian need and/or organization working in response to the humanitarian crisis will be featured on the UAB Institute for Human Rights’ blog.
On October 21st, the thunderous crack of tear gas grenades echoed throughout the streets of Chad as palls of black smoke billowed into the horizon. The security forces in Chad’s two largest cities,Moundou and N’Djamena,indiscriminately opened fire onto an anti-government protest. About 50 people were killed and nearly 300 injured in violence that broke out in response to the delaying of the country’s transition towards civilian rule. Hundreds of protestors took to the streets to demand a quicker transition to democratic rule.They were met with internal law enforcementusing tear gas and firing live ammunition to disperse the protest. Protesters threw stones;some unverified photos showed a fewindividuals with knives, but no evidencewas found to indicate that protesters carried guns.It began with demonstrators advancing despite policereleasing tear gas. However, once the police opened fire, demonstrators were forced to flee, with some helping to carry away the injured and dead. Saleh Kebzabo, the prime minister, announced the death toll at a news conference, explaining that the security forces acted in self-defense.
Source Yahoo Images
Chad’s political background
In April 2021, President Idriss Deby died after three decades of iron-fisted rule, sparking a period of political turmoil in the vast, military-run Central African nation of Chad.Mahamat Idriss Deby, his son, seized power shortly after the coup and promised that elections would take place after an18–month transitional period. However, on October 1st, he postponed the democratic elections by 2 years.October 21st would have marked the end of the initially agreed 18-month transition period,which is why oppositional groups decided to hold the protest that day. The military junta serves to incite the underlying political challenges facing Chad. With a rise in extremist violence and deep social problems, Chad hasrecently seen a series of coups d’états.
Source Yahoo Images
Global Responses
The Office of the High Commissioner for Human Rights(OHCHR) condemns the repression of demonstrations that led to deaths in Chad.Ms. Shamdasani, spokesperson for OHCHR stated that“Defense and security forces must refrain from the use of force against peaceful protesters and ensure that force is not used unless strictly necessary and, if so, in full compliance with the principles of legality, precaution, and proportionality.” Lewis Mudge, Central Africa director at Human Rights Watch, concurs, “People should be able to peacefully protest government policy without being shot at or killed.”The International Federation for HumanRights(FIDH) and its Chadian organizations, the Chadian League for Human Rights (LTDH) and the Chadian Association for the Promotion and Defense of Human Rights (ATPDH) have called for an immediate end to the violent repression of the demonstrations taking place in N’Djamena, Sarh, Doba, Koumra, Abeche and Moundou by the defense and security forces. No longer can the impunity enjoyed by the Chadian transitional regime endure.
Human Rights Violations
What is going in Chad is a violation of human rights that threatens all of us.The preservation of human rights is imperative since these rights protect vulnerable groups as well ashelp fight against unjust cultural and religious practices that infringe on the rights of individual citizens. As a society that treasures the sanctity of human rights, we havea duty to be watch–dogs that safeguard these rights so that all rights, including ours, are protected. Article 19 of the United Nations Declaration of Human Rightsguarantees everyone the right to free speech. Violence against unarmed protesters is not tolerable. Access to the democratic election process is the cornerstone of modern state governance. By deciding who governs, elections give citizens a voice in their government in the most fundamental way. Protecting voter rights preserves the integrity of the election, and therefore legitimizes government. A government without legitimacy is a failed state that cannot accomplish anything.Chad has a responsibility to its citizensto protect and respecttheir rights to peaceful assembly, freedom of expression, and freedom of opinion. Although conflict has been a regular feature since the country’sindependence, these protests are the culmination of the current mixture of internal volatility and factionalism.Anyone who lives in the free world and values their liberty should be concerned for their own rights.It is important for Chad’s international partners to support civil society so that they can reduce violence risks and promote human rights.The deadly aftermath should serve as a harrowing reminder that our own human rights are in jeopardy if this situation is not remedied.
UAB is an Equal Employment/Equal Educational Opportunity Institution dedicated to providing equal opportunities and equal access to all individuals regardless of race, color, religion, ethnic or national origin, sex (including pregnancy), genetic information, age, disability, religion, and veteran’s status. As required by Title IX, UAB prohibits sex discrimination in any education program or activity that it operates. Individuals may report concerns or questions to UAB’s Assistant Vice President and Senior Title IX Coordinator. The Title IX notice of nondiscrimination is located at uab.edu/titleix.