Today is the 50th anniversary of Dr. Martin Luther King, Jr.’s tragic death. It is imperative we reflect on his contributions as a civil and human rights icon while working together, in these trying times, to pursue Dr. King’s dream. This blog, the first in IHR’s MLK, Jr. 50 series, commemorates Dr. King’s commitment to economic and social justice by describing the events preceding his assassination in Memphis, Tennessee.
On February 1, 1968, two Memphis Department of Public Works garbage collectors, Echol Cole and Robert Walker, were crushed and accidentally killed by a deficient truck. In the following weeks, amid repetitive neglect from the city, 1,300 black men representing the department went on strike. One of the garbage collectors, T.O. Jones, took on the role as a union organizer, alongside American Federation of State, County, and Municipal Employees (AFSCME) president Jerry Wurf, demanding union recognition, improved safety standards and a better wage.
Though the sanitation workers were granted a charter in 1965 by the AFSCME, a 1966 strike that addressed usage of out-of-service trucks and overtime pay was foiled by then-mayor Henry Loeb. On February 11th, 700 men attended a union meeting, ultimately deciding to go on strike and, within a week, the local branch of the National Association for the Advancement of Colored People (NAACP) officially supported their efforts. On February 22nd, a sanitation worker led sit-in provoked a City Council vote to recognize their union. However, under Mayor Loeb’s authority, this vote was rejected.
After Mayor Loeb’s controversial decision, a nonviolent march to City Hall led resulted in local police challenging demonstrators with mace and tear gas. This event generated a meeting between 150 local religious leaders, where they formed the Community on the Move for Equality (COME). COME was a nonviolent disobedience collective, led by Dr. King’s ally James Lawson, designed to fill Memphis jails and create attention for the sanitation workers’ plight.
After being updated by Lawson over the phone, Dr. King arrived to Memphis on March 18th and spoke to a crowd of nearly 25,000, the largest indoor civil rights gathering at the time, where he exclaimed, “You are demonstrating that we are all tied in a single garment of destiny, and that if one black person suffers, if one black person is down, we are all down”, encouraging a citywide sanitation work stoppage.
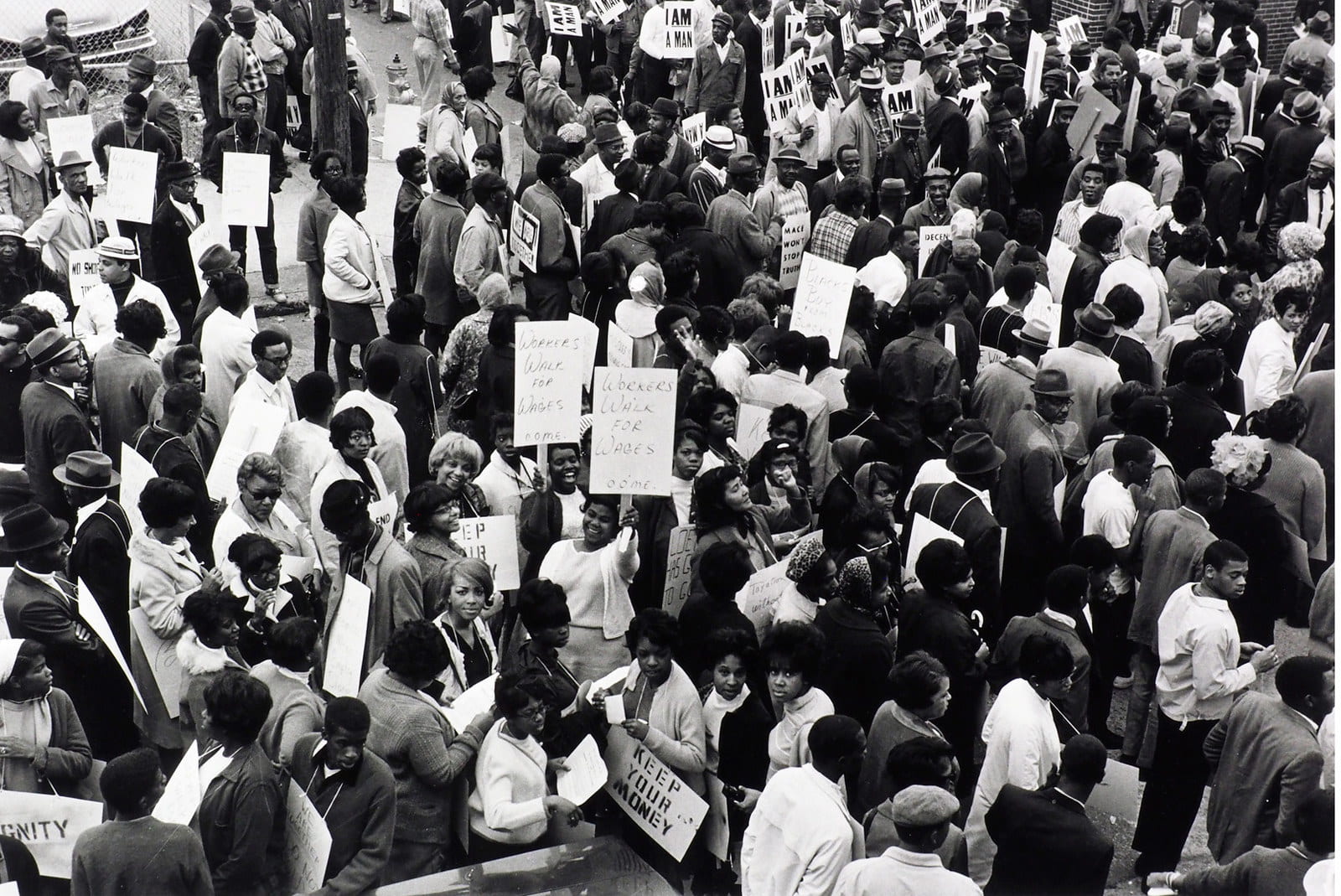
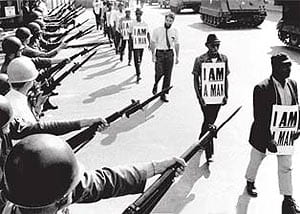
On March 28th, thousands of strike supporters and Dr. King attempted to march, but violence promptly cut the event short. This was followed with shop looting and the murder of a 16-year old by a police officer. Though Dr. King sought refuge in a hotel, many of the marchers fled to Clayborn Temple where police released tear gas into the place of worship and proceeded to club disoriented activists. Subsequently, Mayor Loeb declared martial law, leading to the deployment of 4,000 troops from the National Guard. However, avoiding discouragement, over 200 striking workers marched the following day, holding the acclaimed “I Am A Man” protest signs.

Back at his home in Atlanta, working on the Poor People’s Campaign, Dr. King considered not returning to the chaos in Memphis, but, in the name of successful nonviolent struggle for economic justice, decided he must. Reluctant to invite Dr. King, the Southern Christian Leadership Conference (SCLC) agreed to welcome him back on April 3th where he presented his legendary “I’ve Been to the Mountaintop” speech, declaring, “We’ve got to give ourselves to this struggle until the end. Nothing would be more tragic than to stop at this point in Memphis. We’ve got to see it through”. The following evening, Dr. King was assassinated on the balcony of the Lorraine Motel, leading to national mourning and despair.
Under scrutiny from this tragedy, President Lyndon Johnson ordered his Undersecretary of Labor to negotiate a deal with Memphis leaders to end the strike. Soon after, on April 8th, 42,000 people, led by Dr. King’s widow, Coretta Scott King, SCLC and union leaders, marched to City Hall where AFSCME pledged to support the sanitation workers until the bitter end. On April 16th, negotiations finally allowed the City Council to offer the union a deal, finally ending the 65-day strike and guaranteeing sanitation workers a better wage.
Over the past 50 years, the progress made in Memphis of 1968 has served as a microcosm of labor rights accomplishments across the nation. However, the current U.S. political climate threatens these achievements by decreasing the number of Occupational Safety and Health Administration (OSHA) inspectors, rolling back public reporting of workplace deaths, removing paycheck transparency and banning forced arbitration clauses for sexual and discriminatory violations.
Reflecting on the Memphis sanitation strike demonstrates how the voice of a generation helped intensify one community’s plight, though it is also a testament of how ordinary people can successfully advocate for social justice when they believe “we’ve got to see it through”.