The Carter Center was founded by the 39th president of the United States, Jimmy Carter. The Center advocates for the different faces of human rights. Programs are focused on health, politics, and peace. The Center collaborates with numerous organizations, like the CDC and WHO, to implement programs in countries willing to better the lives of their citizens. At the Center we met with Lauren Kent-Delaney, who is the educational director. She introduced the overview of the center and the many educational opportunities for college students like ourselves.
One important program of the Carter Center is the Guinea Worm eradication program. We met with Dr. James Zingeser, senior project advisor for the Guinea Worm eradication program, and he taught us about the successes and further challenges for the program. The program has been very successful in eradicating guinea worm in humans; however, the program is now facing a new challenge after the discovery that frogs may be a paratenic host, and may be passing the larvae to many animals such as dogs and baboons, which may be perpetuating the guinea worm.
With this being our final stop on our road trip, we were able to see many of the underlying themes of the Guinea Worm Eradication Program connect with what we have learned throughout the past 2 weeks. In order to be as successful as they are, the program had to gain the trust of each community they visited. They did this by working with community members and by giving them tools to prevent and contain the spread of the disease. Dr. Zingeser mentions how adequate communication is vital to keep the trust among the community and how it is hard to gain the trust, but easy to lose it. During our visit to the Veterinary School at Auburn, we learned about One Health, which can be applied to the guinea worm program and how relevant it is to understand our connection to our environment and everything in it.
Dr. Zingeser says that we are smarter together. This quote highlights how it is essential to bring all the various fields together in order to achieve health equity, to overcome social determinants of health, and to work in harmony towards the needs of population health.
Grady Memorial Hospital, founded in 1890, continues to have a significant presence in the city of Atlanta. Those born in the city often refer to themselves as “Grady babies”, an endearing term that comes with a certain sense of pride. This respect stems from the rich history of Grady Memorial and Atlanta as a whole. The hospital is the Southeast’s largest Level 1 trauma center and they are committed to providing quality care for the residents and underserved people of metro Atlanta and Georgia.
Grady Memorial doesn’t turn anyone away. They provide healthcare for all of their patients, including those who cannot pay or don’t have health insurance. Dr. Arthur Yancey, Medical Director for Grady’s EMS Emergency Communications Center, told us about Grady Memorial’s six neighborhood clinics and their Mobile Integrated Healthcare Unit (MIHU). Clinic services focus on treating patients the moment they come in contact with them, and the MIHU focuses on working with high risk patients to reduce the costs associated with hospital readmissions.
On Homelessness
Homelessness is so much more than the stigma that surrounds it. Many believe that the homeless are those who roam the streets; however, this is a biased notion. Not having a roof over one’s head does not equal homelessness — an unstable home does. Atlanta’s increasing homeless population stems from the city having the highest level of income inequality in the U.S., giving way to their inclusive free healthcare system.
According to Emergency Medicine Physician and Medical Anthropologist Dr. Bisan Salhi, it is easier to bring someone from the brink of death than to get them the housing and food security assistance they need in the community. Our social welfare systems and healthcare systems are designed in such a way that our emergency lifesaving treatments are often more available than basic social services. Resources hard to coordinate for patients include transportation, healthy food, and housing. However, there are many social determinants that keep vulnerable populations from reaching the best possible health outcomes. Dr. Salhi defined social determinants simply as, “the easier and better your life is, the better your health outcome is.” Therefore, if you live in an area with more availability to resources, your health outcomes will be better than those who are restricted.
The Georgia Poison Center is a free and valuable resource for Georgia’s communities. It is part of a national network of poison control centers around the country. These centers are invaluable resources during toxicological emergencies and can be an early warning and surveillance system for contamination events or disease outbreaks. Poison control centers are an economic investment as every dollar invested in them saves $20 in healthcare costs. The Georgia Poison Center is funded by both state and federal sources and works closely with the Georgia Department of Public Health. They are a busy center as they receive up to 100,000 calls per year. Given the medical cost savings and the number of individuals that are assisted, it was noted that each state would benefit from a poison control center.
Dr. Ziad Kazzi, an emergency medicine physician and medical toxicologist at Grady, met with us and made reference to several interesting points about the more commonly ingested products including e-cigarettes and vaping fluids, laundry detergent pod ingestion, and even asphyxia from the inhalation of helium from balloons. Another emerging issue is stemming from the legalization of marijuana and the dangerous effects it has had on children that accidentally consume edible products with THC. This shows the importance of poison control centers and the need to preserve them to protect the future.
Everyone is familiar with the CDC, a looming government institution even featured in pop culture shows such as The Walking Dead. But unless you work there very few people get to experience the magnificence first hand. It was very interesting to see all of the advancements in science throughout the iterations of the organization itself. From focusing on malaria and venereal diseases to now administering surveys and programs concerning exercise to name a few. After touring the CDC museum, which details not only public health advancements of the last 100 years or so and features recent extensive outbreak work battling Ebola, we met with UAB School of Public Health alumni. Meeting with Ivy Singletary, MPH , Margaret Paek, MPH, and Dr. Leigh Willis was an illuminating experience for many of us who wondered exactly how the CDC and all of its many interlocking pieces truly fit together. One of the things that really stuck out to us was the diversity in not only the work that they do but the sheer amount of opportunities awarded by the CDC. Just like any organization there is always some resistance when trying to get new projects up off the ground, but according to our alumni the best traits for public health students to cultivate are to be flexible and resilient.
Despite resistance, one alumnus, Leigh Willis, PhD, was able to create and enable a whole new method of outreach in order to share good health practices with the public. The method he pioneered at the CDC was Motion comics. https://npin.cdc.gov/KABIChronicles/index.html Not only is the program available to the public, but discussion guides come with each video to allow for interactive learning between participants and facilitators. Perhaps one of the keys to success is doing your research and presenting your supervisors with a product, rather than just an idea. Both Ivy and Margaret suggested to us that this was a key to having projects and programs picked up and funded. If you put in the work, and show that you have the initiative, you are more likely to get suggestions on how to improve. The experiences of these alumni gave us a realistic view of working at the CDC and increased motivation to serve in the field of public health.
Every time you go to the grocery store, a restaurant, or school cafeteria, you can trust that you are eating safe food thanks to the dedicated staff at the state diagnostic laboratories. These scientists are responsible for disease surveillance, testing, and regulation of livestock, poultry, wildlife, and even honey bees. Dr. Frazier and his staff test and monitor domestic and wild animals for emerging and foreign diseases as well as diseases that can be passed from animals to humans: zoonotic diseases. The Alabama State Diagnostic Laboratory collaborates with the Alabama Department of Public Health on the surveillance of zoonotic disease. Human health and animal health interface on a daily basis as people interact with family pets, farmers interact with livestock, and feral animals cross human paths in urban, suburban, and rural areas. To assure that humans are healthy, the animals that share our environment must be healthy and visa versa. The term “One Health” encompasses the collaboration, cooperation, and communication between veterinary scientists and public health professionals to maintain a strong and thriving environment.
Our Wednesday began outside the Alabama Animal Diagnostic Laboratory were we had a spontaneous conversation with Dr. Tony Frazier, the state veterinarian with the Department of Agriculture and Industries. Cloaked within his humorous banter were some powerful truths: “A country that has lots of food has a lot of problems. A country that has no food has but one problem. Agriculture touches everyone’s life. Food and food safety is important for everyone” As public health students, we don’t often think about how agriculture intersects with our work. We weren’t sure what we’d learn and what we’d see inside the lab. We were in for quite a surprise!
In the pictures below you can see us suited up in personal protective equipment before we entered the part of the diagnostic lab that houses the “Digester”, a large piece of equipment used to safely dispose of animal tissue and bone after its been necropsied and tested. This disposal procedure prevents the spread of harmful zoonotic diseases.
But it wasn’t all fun and dress-up games for the UAB Trailblazers. Dr. Frazier opened our eyes to the various avenues in which human health depends on animal health and visa versa. Did you know that Alabama has an enormous industry? We didn’t! And since the southeast is prone to hurricanes and tornadoes, the state has emergency preparedness protocols in place to assist when farmers suffer loss in the case of a natural disaster, or should a deadly disease be introduced to a chicken house. We learned from Dr. Heather Waltz, Director of Animal Diagnostic Lab, that part of the lab’s role is to monitor livestock populations at several points before they go to be “processed” and eventually sold in supermarkets. The lab runs thousands of tests on behalf of producers and consumers. Dr. Kelly Steury, DVM, MPH, Diagnostician and a recent alum of the SOPH spoke about emerging zoonotic diseases, including bovine sponginess encephalitic (mad cow disease), and the convergence of animal and human health.
As students of public health we keep finding we also must be students of history. Dr. Stephanie Ostrowski, Associate Professor of Public Health at the Auburn University’s College of Veterinary Medicine, detailed what could be considered the worst epidemic in history, although it’s not well documented: the Rinderpest plague of the late 19th century. The virus is structurally similar to measles, but can’t be transferred from animals to humans. In 1884, cattle imports introduced rinderpest, a virus known as the cattle plague, into Ethiopian herds of cattle and oxen. One hundred percent of cattle exposed to rinderpest contract the disease and more than 99% of infected cattle die of the disease. This epizootic event in Ethiopia annihilated livestock leading to the Great Ethiopian Famine of 1888-1892. Around 30% of Ethiopia’s population starved or died from other consequences of rinderpest. It spread from Ethiopia to other parts of the African continent, destroying livelihoods and causing economic disenfranchisement along the way. This likely made it much easier for colonists to continue to invade and oppress African people. During the 20th century, rinderpest was eradicated throughout the world by vaccinating cattle herds. However, much can be learned from the events and impacts of the rinderpest disaster of the 19th century. Most of us were unaware that this had even taken place. This historical tragedy highlights the connection between human health and animals, even when the disease itself can’t be transferred from animal to human.
Our day transitioned into a tour of the Auburn University College of Veterinary Medicine’s (AVM) state of the art facility that focuses on the prevention of many diseases and conducts comparative medicine research. While at the AVM, Dr. Jim Wright, Professor at AVM, discussed how vital controlling rabies is for population health because infection in humans almost always results in death. We learned that the Alabama Department of Public Health is at the fore front for monitoring cases of human rabies and track the animal source. Animal sources are not just limited to wildlife, as companion animals can be infected with rabies as well. AVM’s collaboration with other research teams (including UAB!) develop innovative projects that focus on some of the most prevalent diseases. Their collaborations embody the mission of One Health, by demonstrating that animal health is vital to improving the livelihood of populations.
Dr. Wright left us with a memorable approach to public health that will help us indicate when something needs attention: “Embrace the enthusiasm of looking at something weird.”
“History, despite its wrenching pain cannot be unlived; but if faced courageously, needs not be lived again” – Maya Angelou
Among the green pastures and businesses in Tuskegee lies a strong historical foundation. Tuskegee is a community deep rooted with faith, resilience, and forgiveness. It was these things that pulled them through the 40-year syphilis study that started out as a treatment program with good intentions, with funding from philanthropist Julius Rosenwald, and morphed into a unethical experiment that not only harmed the participants and their families, but also violated the trust of the community.
Trust is the foundation in which public health is set upon. This was known by the researchers and scientists involved in the United States Public Health Service’s Tuskegee Study of Untreated Syphilis in the Negro Male. They needed a connection to their target community; therefore, Nurse Rivers was the perfect bridge to that audience. Nurse Rivers was an African American women deeply rooted in the Tuskegee community as she had served as the communities public health nurse. They trusted and respected her fully; therefore, she was key to recruiting those with “bad blood” into the study.
On Health Equity
How do researchers help ensure the safety and rights of research participants? Through informed consent, which is when research participants understand the potential benefits and risks involved in the study. Dr. Stephen Sodeke, a bioethicist and professor of allied health sciences at Tuskegee University’s National Center for Bioethics in Research and Healthcare, defined bioethics as “identifying and addressing ethical, social, religious, and legal issues that arise in medicine, research, public health, and environmental science.” However, for the African American men of the Syphilis Study there were no such laws in place that discussed consent. Dr. Jontyle Robinson, the curator of the Tuskegee University’s Legacy Museum, introduced the case of Henrietta Lacks during our visit to the museum. Ms. Lacks nor her family, had any idea that cells had been taken from her body or used in research. “HeLa cells” derived from Ms. Lacks, have been used in countless research studies and even used to help create the polio vaccine. This does not negate the fact that the doctors should have gotten her permission before extracting her cells.
On Population Health
Felicia Chandler and her family took the time to discuss with us their memories of the Shiloh-Rosenwald School and how their community was targeted during the Syphilis Study. The motto of the school was”good, better,best, never let it rest, never stop until the good is better and the better is best”. Through Mrs. Chandler and the others that talked with us, this motto shows us a glimpse into the educational values instilled in the community. They are a close-knit, resilient community strong in faith and even stronger in facing adversity. Looking back, they feel that the U.S. Public Health Service unfairly deemed the people of their community as ignorant, poor and uneducated; and as such were made to feel unvalued and less than human. The people of this community worked hard, educated their children when African Americans could not attend public school, were land owners, with many of their residents continued on to do great things for this country. The Tuskegee Syphilis Study has had a lasting negative impact on the community as well as a general and deserved mistrust of the government and outside medical professionals. This study left residual trauma that is still felt today and perpetuates health inequities.
Our Final Thoughts
Considering all that we have learned today, a major theme to recognize is that each one of us is a “piece” of a jigsaw puzzle. Whether you are an educator, policy maker, or medical professional, together we are like a puzzle. We must figure out how to connect, raise awareness, and give vulnerable populations a voice. We need to carry all the lessons that we have learned, and apply them as we progress in our future professions and combat the adversities we are still witnessing today.
During this visit, we learned about the Alabama Department of Health’s (ADPH) Southwestern Health District. This district includes the following counties: Baldwin, Choctaw, Clarke, Conecuh, Dallas, Escambia, Marengo, Monroe, Washington, and Wilcox (see the image below for a graphic representation). It may seem odd to you that Mobile county is not included in this district, as it is so geographically close. However, both Mobile and Jefferson counties operate somewhat independent health departments and as such, have become their own districts.
The Southwestern District is largely rural with median household incomes per county ranging from ~51K (Baldwin) to ~24K (Wilcox). The percentage of folks who live in poverty ranges from 11.7% (Baldwin) to 35.4% (Dallas). Baldwin has a higher socio-economic status than the other counties due to its lower half being a great destination for tourists and people who want to live by the beach. Dallas and Wilcox Counties are primarily African-American (70%). Naturally, we wondered how the Southwestern District Administrator addressed the diversity between counties with regard to income, poverty, race, and other social determinants of health.
Luckily, we had the opportunity to sit down with the District Administrator, Chad Kent, the Assistant District Administrator, Suzanne Terrell, and the Director of Field Services for ADPH, Ricky Elliott. We met them at the Escambia County Health Department and learned about the many programs and services offered at each of the local health departments, like the one we were in, throughout the District. These programs included, but were not limited to family planning, sexual health screening (STI and HIV testing), lead screening, home health programs, cancer detection programs, and diabetes education. Some counties even offered additional maternity services and included peer breast-feeding educators. We were also surprised and grateful to hear that in one county, the social worker actually brought birth control to a client who had no transportation. While this was likely an unlikely occurrence, the compassion of the local health department staff for their communities and their willingness to go above and beyond the call of duty does not go unrecognized.
The commitment of the staff of the Escambia County Health Department and the Southwest District to their residents is impressive, especially with their dedication to make healthcare accessible to all that live here. While we were discussing this with them they shared with us a story of an elderly couple who would have had to drive over three hours one way to see a nephrologist at UAB. The trip was difficult for the couple; navigating Birmingham’s traffic and parking was a source of great stress. Through ADPH’s Telehealth Program, this couple and others can now “meet” their doctor at their local public health department. Doctors can communicate with patients via a video call during routine follow-ups. Some conditions can even be diagnosed and treatments recommended via this technology. This program is breaking down transportation as a barrier to accessing the care their residents need in order to live healthy and active lives.
While Telehealth is certainly a technological achievement, the District leadership was also very excited about two new changes coming to the District (and the state). First, a new electronic health record (EHR) system will be implemented later this year. An EHR system will allow for greater continuity of care within the ADPH system, as well as increase the ability to communicate with other providers. Second, Women, Infants and Children (WIC) is going somewhat digital as well. Traditionally, WIC clients have received vouchers that they can turn in for certain goods at their local retailers. Soon, WIC clients will receive a WIC card that will be loaded with a certain amount of money to purchase WIC items. This eWIC program enables clients more flexibility in the WIC items they can receive, saves time, and reduces any voucher and low income related stigma. Additionally, data from purchases will be used to inform other WIC services moving forward. Overall, technological advances have really increased the ability of ADPH to learn from their communities and adapt to better meet their needs.
The UAB Public Health Trailblazers headed to Atmore, AL after a restful but educational weekend. Our class includes students with heritage from most continents, and even some with Indigenous American heritage, but none who grew up in a tribal cultural setting. We were all outsiders as we entered the Poarch Creek Band of Indians. We were there to visit the new tribal health department and health center and to meet with Sandra Day, the Director of Community Health.
Since our readers, like all of the student Trailblazers, probably would benefit from a brief background of this tribe’s history:
It is well established that the European settlement of North America led to various forms of systemic oppression, relocation, and genocide to the indigenous people that were here. In 1830, the Indian Removal Act forcibly relocated southeastern tribes to federally owned land west of the Mississippi River. The Poarch Band of Creek Indians circumvented this relocation and continued to reside in south Alabama, mainly in Escambia County. They became a federally recognized Tribe in 1985. Although the acceptance of tribes across the United States has improved, the negative impacts of long term oppression still resound within tribal communities. As much as we’d like to think of this discrimination as ancient history, we must face the harsh realities of what happened not so long ago so that we can work towards genuine equity.
Native Americans experience higher rates of chronic liver and respiratory diseases, assault and homicide, self-harm and suicide, and alcohol and drug abuse when compared to white communities. The Poarch Band of Creek Indians Tribal Health Department is working to decrease these health disparities through access to services, health education, and several specific grant programs.
One such grant is the Good Health and Wellness project sponsored by the United South & Eastern Tribes (USET) and the Centers for Disease Control and Prevention (CDC). Mrs. Wynell Bell, the grant manager, detailed some of the programs they have implemented to address diabetes, obesity, and hypertension – the top three health indicators affecting their tribe. Incentives encourage the use of a monthly farmers market on the reservation. Wellness Wednesday is an event for the whole community, young, old, and in between, to survey individuals’ health and engage elders in physical activity. “They value their youth, and they value their elders,” Day told us. This event brings both together in a fun interactive event to pursue better health. As a reward for participating, vouchers for the farmer’s market (another result of this grant) are handed out to attendees.
Despite the efforts of the Poarch Creek Health Department, the tribe faces numerous barriers to improving their health. After a history of discrimination, distrust for nontribal members resonates throughout. To this day, the reservation remains a food desert. After elevated disease rates lower life expectancies, tribal members accept fatalistic perspectives toward health. The history of the Poarch Band of Creek Indians has shaped their health outcomes, but the devoted employees at the tribal health department remain optimistic. Programs that rely on grant funding are hard to sustain once the funding dries up. According to Bell, “this does not deter them from providing evidence-based programs and services that will work to improve health outcomes over time”.
It was very apparent from our visit that this community is completely family-oriented. We could feel it. And as we departed, we were left asking ourselves how can we reach out to help a community with a history of distrust of outsiders? How can we encourage young tribal members to seek training in medicine and public health and return to the reservation in order to improve health in their community? These and many other questions weren’t answered in a day. We won’t find a one-size-fits-all solution. Nor can we work in isolation; it will take a collaborative approach from many people from different sectors to provide comprehensive solutions. For the Poarch Band of Creek Indians, improved health outcomes can be achieved by programs that involve the whole family and partner with other organizations to seek common goals. With every stop, we gain a deeper understanding of how essential collaboration, trust, and community-focus are for achieving greater health equity.
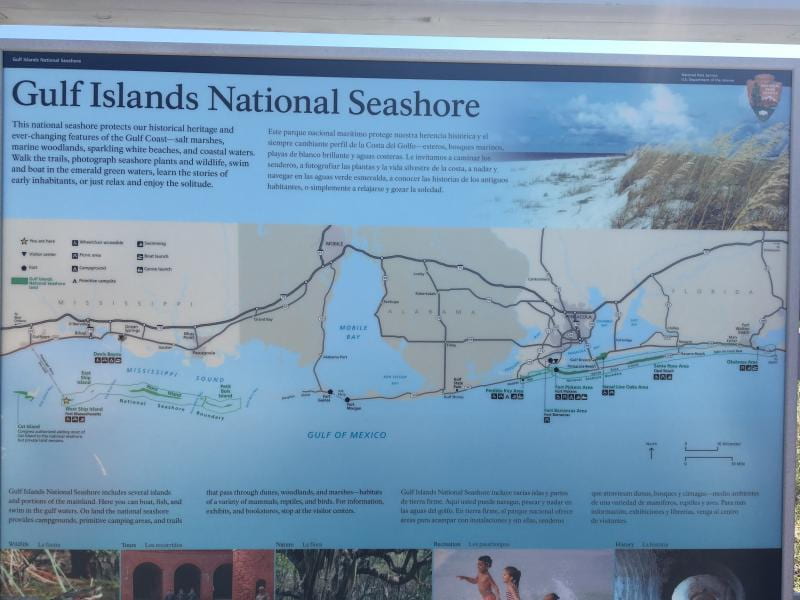
After a week of excursions throughout the Deep South, we spent our Saturday on Ship Island, at a popular and historical destination off the coast of Biloxi, Mississippi. Discovered by the French in 1699, Ship Island was considered the “Plymouth Rock” of the Gulf Coast. Fort Massachusetts, which played a role in the civil war, is located on the island and housed one of the nation’s first quarantine stations beginning in the 1870s. The quarantine station operated at the height of the yellow fever epidemic and monitored vessels, cargo, and passengers as a first line of defense into the Port of New Orleans. Today, the island does not look like it previously did due to damage left from the impacts of Hurricane Camille in 1969.
After an hour and a half on the boat known as “Captain Pete”, we arrived on West Ship Island, home of Fort Massachusetts. Our initial purpose was to search for plastics and microplastics along the beach; however, the park ranger informed us shortly after arriving that two other academic groups had beat us to it leaving no plastic in sight! We did notice a few measures the National Park Service is taking to protect the environment on the island including handing trash bags to visitors upon arrival and having receptacles for people to deposit trash as they leave the beach. The island is also known as a Least Tern nesting area. A large majority of the islands sandy shores are roped off for these seabirds so that they can nest in peace. Park Rangers were clear that heavy fines will be leveed to anyone that ventures into those areas.
Even though we weren’t able to recover plastics from the seashore while on the island, we were able to address an equally important public health issue…mental health and self-care. As students, we know how it feels to be overwhelmed by stress and visiting places like Ship Island is a great way to de-stress and just have fun. We saw families and friends of all ages spending quality time together and building new memories on this historic island.
So remember matey’s, always reduce, reuse, and recycle your plastics and even pirates need a day off.
“How did this happen?” “Is this America?” These are the contemplative
and persistent questions that come to mind while walking through the Katrina
Exhibit at The Louisiana State Museum. The exhibit is housed at The
Presbytère, an eighteenth-century architectural gem on Jackson Square in New
Orleans. It has been nearly thirteen years since Hurricane Katrina hit
the city of New Orleans, but time stands still as we walk through the
exhibit. The exhibit opened in 2010 and features eyewitness accounts,
historical artifacts, interactive exhibits, and historical as well as
scientific information on hurricanes, geography, and the levee systems.
The museum was created to provide an educational experience highlighting the
failed processes that led to the magnitude of the disaster and emphasizes the
efforts toward recovery. The museum inspires its visitors to think about
the importance of mitigation, preparedness, and response operations and the
relationship between poverty and disaster outcomes.
The Katrina Exhibit was designed to answer questions posed at the beginning
of our blog. From a public health perspective, it is important to
evaluate the effects of hurricanes and how they impact the health and
livelihood of a community. To quote the philosopher, George Santayana,
“Those who cannot remember the past are condemned to repeat it.” The
exhibit describes the history of larger hurricanes that have impacted
Louisiana. After learning of Hurricane Betsy, a.k.a Billion Dollar Betsy, our
group recognized post-disaster outcomes (e.g. disease, injury, death) and how
these outcomes can be exacerbated by poverty and not having effective emergency
protocols and mitigation systems in place. The exhibit showcases
photographs and personal stories of the destruction which can be prevented in
future storms.
Katrina was not a discriminatory storm and affected all in her path.
The aftermath of the storm left immense environmental impacts. As public
health students, we recognized the social determinants of health while reading
through the displays. There are too many facts presented in the exhibit
to mention in this blog, but there were a few memorable stories that stood
out. Seats from the Superdome were displayed to represent the shelter
that was used at its height for 35,000 people. The living conditions
within the Superdome were unfathomable with stifling temperatures, filthy
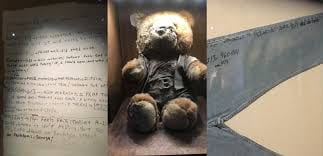
conditions, and a disgusting stench. Another display features the diary
of a gentleman, the late Tommie Mabry, who wrote about the conditions he
experienced while stranded at his home. His memories are somber to read
with his thoughts on survival, his thankfulness for friends and neighbors, and
how he kept busy during the period following Katrina. Furthermore, Mr.
Mabry wrote about being unwell and his worries about not having access to
healthcare. Both of these displays from the exhibit are demonstrative of
how the residents of New Orleans suffered.
“The Hurricane was fair, we were all affected, all devastated. The aftermath
was not, the resources were not, the breaches were not. It was an injustice.”
Over a span of thirteen years, many efforts have been dedicated to social,
economic, environmental, and infrastructure recovery in New Orleans. The former
mayor, Mitch Landrieu, declared in 2017 that New Orleans is “no longer a
recovering city, but a city that has recovered and is now moving forward.” Some
community members beg to differ. Many residents believe that New Orleans
has a long way still to go.
There have been improvements. New evacuation policies, procedures and
routes have been put in place for quicker evacuation of residents from the
city, including those with disabilities and lack of transportation. Statues
have been erected that mark evacuation points throughout the city were people
can congregate to board buses to be evacuated out of the city in an emergency.
Despite mistrust in the city towards the Army Corps of Engineers and the Flood
Protection Authority, new and improved levee systems have been put into place.
However, we learned through an interactive display at the Katrina Exhibit that
nothing can mitigate storm surges in southern Louisiana better than the natural
protection of marshes and swampland. However, this barrier is slowly disappearing.
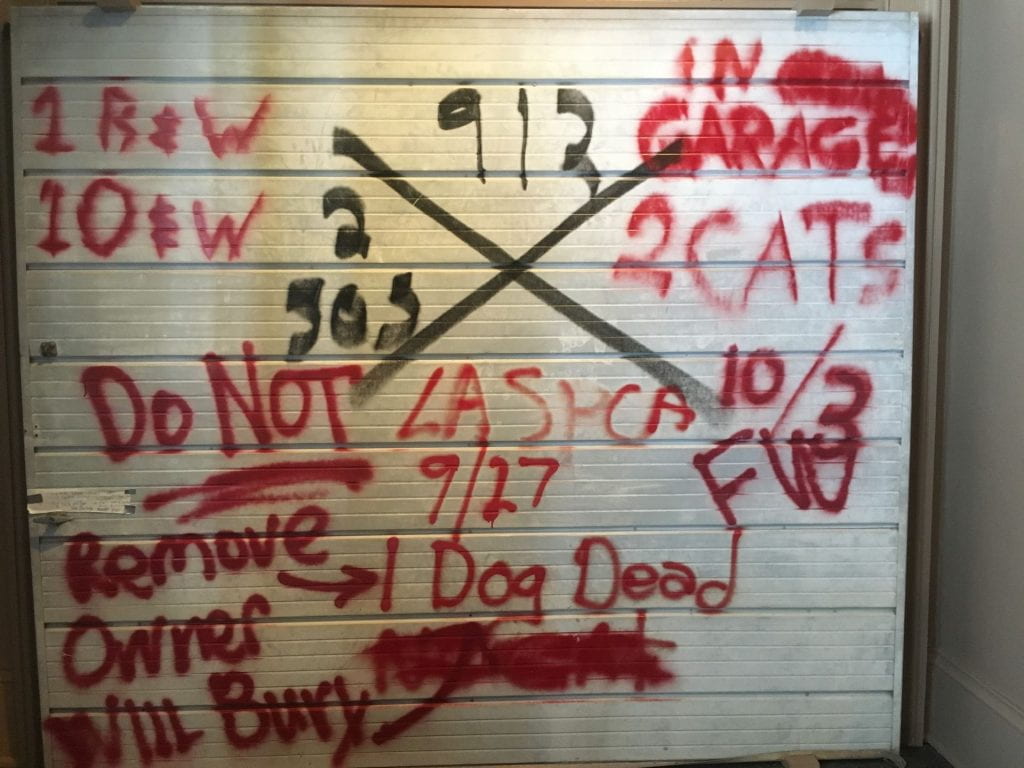
The Lower Ninth Ward had some of the most traumatic effects from the storm.
Homes were swept away, knocked off their foundation, and some residents were
found drowned in their attics. On top of being a low-income neighborhood,
Katrina left the community groveling for help and resources. The neighborhood
is primarily African American and historically was the first neighborhood where
African Americans could own homes. Many of the homes in the community have been
passed down through the generations and very few had homeowner’s or flood
insurance.
In a speech addressing the issues related to Katrina, President George W.
Bush stated, “deep, persistent poverty in this region [with] roots in a history
of racial discrimination…We have the duty to confront this poverty with bold
action.” When disaster struck the Lower Ninth Ward, the neighborhood was
left with very few options on how to move forward. This community was not
financially sound, uninsured, and eight feet below sea level.
With so few options on how to advance, the neighborhood turned to government
support and outside help. We learned of three programs that began after
Hurricane Katrina to help the residents were “The Road Home” program, the “Make
it Right” program, and Habitat for Humanity. Not all programs were
successful or equitable. Director of lowernine.org, Laura Paul, gave us insight
into the rebuilding projects within the community. “The Road Home” project
initially was based on tax appraisal values, rather than the costs of
rebuilding. Homes in the area had not been appraised in the years before
Katrina. So residents were left without the resources to rebuild.
There was a major court case lodged against the program that won. At this
point, however, a lot of the money allocated to the program had already been
spent, so it could not really contribute further to the rebuilding of the Lower
Ninth Ward. The “Make it Right” foundation, founded by Brad Pitt, has accepted
environmentally sound housing designs from all around the world. Using these
designs, various homes have been built within the Lower Ninth Ward. Curtis, our
navigator, who has been driving through the Lower Ninth Ward numerous times
following Katrina, noted the gradual improvements within the community with
each visit. Despite the advancements made in this community, there is still
much to work to be done as evident by the conditions of the road including
inoperable fire hydrants and open storm drains. With the efforts from long-term
disaster recovery organizations, such as Laura’s, hopefully we will continue to
see further development in the Lower Ninth Ward.
Our Daughters of Charity, an organization older than New Orleans itself, and operating within the city for more than half of its history was founded in the 1600s by St. Vincent de Paul. This rural priest became concerned when visiting a sick family that their farm would fall into disrepair and called on his congregation to step up in order to assist this family in maintaining their livelihood while they recovered. Much to his surprise, his community jumped at the offer, showering the family with assistance in the form of food, caring for their livestock, and his idea began to evolve. Through his inspiration the Daughters of Charity were formed in Paris, working directly with the people of their communities where they lived, making an impact by really considering where their patients lived and worked.
The nuns and healthcare providers associated with Our Daughters of Charity lend a hand in many areas of public health and population health, founding hospitals and orphanages in many countries, including the first hospital west of the Mississippi River. With their unyielding focus on community health, this organization has evolved even further to what we see today, hard workers in the Big Easy, establishing comprehensive health centers in underserved areas to fill the gaps left behind, especially after Katrina. In fact, the Daughters of Charity–which is now a recognized Federally Qualified Health Center (FQHC) — is an extensive network of care centers which opened several locations in the NOLA area just one month after Katrina decimated 80% of the healthcare entities in Orleans parish. The organization, lead now by CEO Michael Griffin, a doctoral student in the UAB School of Health Professions, has since opened 10 health centers spread throughout the greater New Orleans area.
The Carrollton Healthcare Facility, in particular, has an interesting renovation story. The current building was formerly a Chase Bank that sat just below sea level. After Katrina, any renovations to buildings over a certain square footage and new buildings had to be built at a higher level. The health center was built around, and above the old bank leading to an interesting series of stairs and elevators to get around the clinic. One hallway even takes you past the old bank vault! What a great metaphor for their work the center does in securing the health and well-being of their clients! Unfortunately, the vault is below sea level and would not be an appropriate safe space during hurricanes or flooding, but it would be great during tornados!
The organization impressively covers a wide array of services in their health centers; adult, pediatric, diagnostic, pharmacy, dental, chronic disease management and prevention, optometry, women’s health, behavioral health, counseling services, and many more. These centers have taken on a Patient-Centered Medical Home (PCMH) designation allowing them some flexibility when working in the best interest of the community. In addition, Our Daughters of Charity has created many community-focused programs to address some of the significant health concerns of the population including diabetes and cardiovascular health. The diabetes program includes a support group for members of the surrounding community. In fact, they were preparing for a meeting with those enrolled in the program while we were there. This program educates participants about their condition and shows them ways to manage their health by providing them with fresh vegetables and other groceries and teaching ways to prepare them in a healthy way. Bags of nutritious foods were already prepared, ready and waiting.
One of the amazing capabilities of Our Daughters of Charity is its electronic medical records system, which is connected to other providers around the city. Staff at Our Daughters are notified if one of their patients checks in to an area emergency department. This ability leads to greater continuity of care and enables staff to identify which patients are having to utilize emergency services most often. This knowledge will be used to prioritize the tasks of newly hired community health workers funded as part of a new Robert Wood Johnson Foundation grant that Our Daughters of Charity has received. Through this grant, the community health workers will be able to identify and work directly with those individuals who frequently utilize emergency health services. Their work will extend into communities to address the barriers their patients have in living a healthier lifestyle. This will truly be an amazing program that benefits the communities through personalized attention.
By the end of our visit, we were truly amazed at the work that Our Daughters of Charity has been and is doing in the city of New Orleans. They are able to maintain their Catholic values while adhering to the federal requirements of being an FQHC and, at the same time, work to meet the needs of the community they serve.
UAB is an Equal Employment/Equal Educational Opportunity Institution dedicated to providing equal opportunities and equal access to all individuals regardless of race, color, religion, ethnic or national origin, sex (including pregnancy), genetic information, age, disability, religion, and veteran’s status. As required by Title IX, UAB prohibits sex discrimination in any education program or activity that it operates. Individuals may report concerns or questions to UAB’s Assistant Vice President and Senior Title IX Coordinator. The Title IX notice of nondiscrimination is located at uab.edu/titleix.