On Monday, May 16, 2022, we had a wonderful time meeting with staff at the Queen’s Nursing Institute (QNI). Establish in 1887 by Florence Nightingale, who paved the way for modern nursing practice and training, the Queen’s Nursing Institute meets the community health needs of the more underserved parts of the United Kingdom population. Based in London, the QNI has an established interconnected network of community nurses that focus on care across the lifespan or “from sperm to worm” as Dr. Crystal Oldman, CBE, Chief Executive Director of the QNI, affectionately describes it. (By the way, we asked Dr. Oldman the meaning of the CBE acronym. CBE represents the Commander of the British Empire. This is the highest-ranking Order of the British Empire award, other than knighthood or damehood. It is given to individuals who have made significant contributions to their field through leadership and service.)
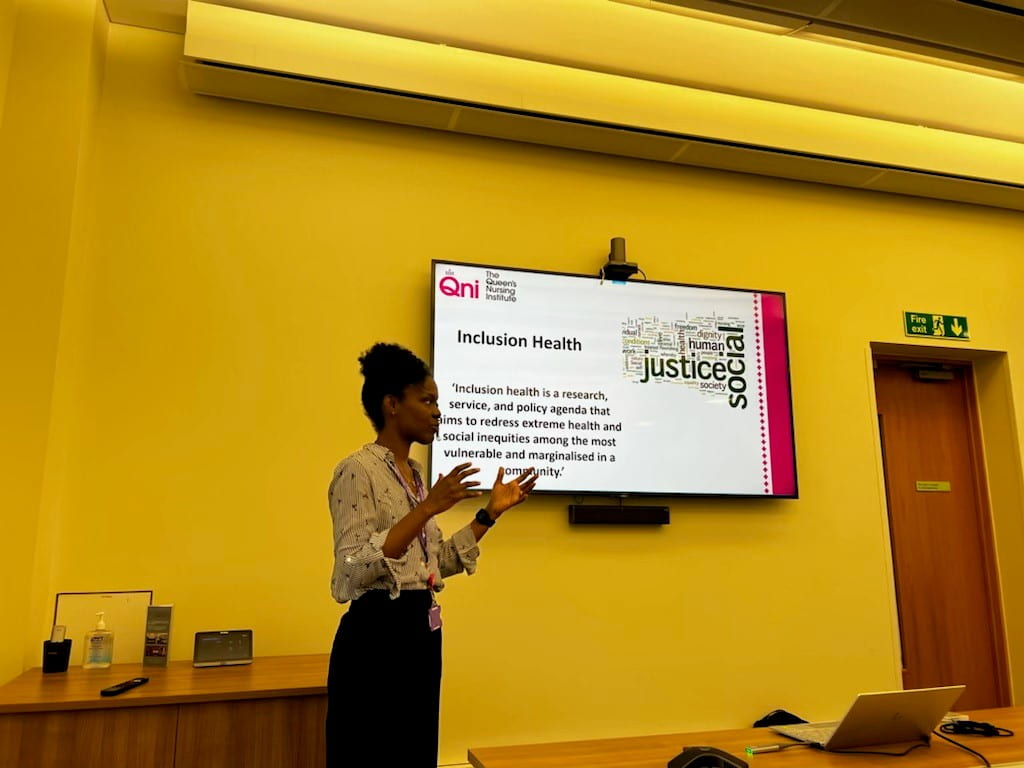
To explore population health and begin to understand some of the integral differences between US and UK population health outreach programs and practices, Kendra Schneller, lead of the Homeless and Inclusion Program of the QNI, provided an overview of her work. The Homeless and Inclusion Health Program supports the identification and meeting the health needs of those experiencing homelessness. In the UK, the homeless definition is broad, including the migrant population, sex workers, asylum seekers/refugees, and those who do not have secured residences of their own. Current and ongoing efforts regarding the homeless population of London’s 32 boroughs that the QNI aims to address include offering personalized health care and connections to a GP for further health needs, resource information for clinicians, and support specialist groups that advocate in support of this population. Their funding comes from a combination of sources including the National Health Services (NHS), acute trusts, and other charitable organizations. Some ongoing struggles to further this program and better meet the healthcare needs of this population include limited funding, lack of housing availability for rehousing, and structural difficulties that allow for transition away from homelessness. Kendra touched upon her hopes for the future, which strongly revolve around additional funding support and fewer institutional barriers.
Moving towards understanding the culture of nursing in the United Kingdom. Rebecca Daniels, one of the first Professional Nursing Advocate (PNA) graduates in the UK’s relatively new PNA program, spoke about the role of PNAs and the current state of affairs regarding nurse wellbeing in the work environment. Practicing based on education from an adapted curriculum of the “Resilience Model of Supervision”, PNAs work to cultivate an environment that prioritizes the mental health and emotional well-being providing a safe space for nurses to release and develop strategies to handle emotionally draining work experiences. The goal is to prevent and better manage compassion fatigue and the general emotional nature of the role—something made apparent during the recent COVID-19 pandemic. Still, in its infancy with only 3000 PNAs currently certified in the UK, the program hopes to certify a net 5000 PNAs by the end of 2022. Daniels spoke about some of the difficulties PNAs face which include resistance from nurses to engage with PNAs because of already dense work responsibilities and obligations. In concluding the discussion, Daniels expressed hope for unifying standards across PNA certification programs to ensure program validity and hope to fully assist nurses in their workplace plights.

Dr. Oldman concluded the presentation with an open discussion about the QNI, NHS, and the greater UK healthcare network. The closing discussion centered around similarities and differences across the current US and UK healthcare including international nursing shortages, a problem verified by the International Council of Nurses (ICN), workplace burnout, and changes wrought by the pandemic. In discussing future directions of healthcare, Dr. Oldman touched upon a need for leaders and advocates from the nursing profession at the forefront of health policy and decision-making:
“If you’re not at the table, you’re on the menu.”


Speaking of menus, following our visit to the QNI, we stopped for a group lunch in the Covent Garden area in London’s West End. While eating lunch, the class noted the conservative use of salt in the UK. Fittingly, Dr. McCormick shared some insightful commentary from Dr. George Howard, Distinguished Profession in the UAB SOPH, who recently read the blog and shared how “the UK has successfully dramatically reduced hypertension through policy changes and partnerships with food companies” to reduce consumer salt intake through processed and prepared foods. This intervention led to a decrease in stroke, hypertension, and related heart disease. Dr. Howard expressed interest in observing outcomes of similar intervention work in the United States to lessen the health burden of heart disease in the Stroke Belt.
It was a lovely day! Stay tuned for tomorrow’s blog update with a visit to the Terrence Higgins Trust and Unilever.
Team 3: Grace Albright, Rachana Kuthuru, and Ritika Samant
