As an immigrant from India who has become an American citizen, food insecurity is something that I have witnessed a lot in my short lifetime. As a kid, I remember seeing people on the streets of India, both young and old, begging for mere scraps, and felt guilty for not being able to do anything to help. Yet, little did I know that I would come to experience similar food insecurities, but in America, a land supposedly filled with life, liberty, and happiness. It was in America that I first became aware of the realities of being poor, and it was here that I learned how to live off of $20 a week.
Among other things that have come into the limelight due to the pandemic, people are starting to pay more attention to the growing food insecurities in America. The United States is one of the most affluent nations in the entire world, yet it is also home to some of the largest food deserts in the world. This phenomenon, which is an incomprehensible reality in one of the richest nations in the world, has only become worse over the past few years, mainly due to the increasing inflation coupled with stagnant wages, which have only been exacerbated due to the pandemic. Food insecurity has become a reality to many Americans who live paycheck to paycheck and struggle to make ends meet, even with working multiple jobs.
Food Deserts

So, what are food deserts and why should we care about them? Well, according to the United States Department of Agriculture (USDA), food deserts are areas in which access to healthy food and groceries is limited due to a number of reasons, including distance, individual abilities, and even the location of the neighborhood someone resides in. Distance becomes an issue for those who live far away from stores that sell fresh produce, including those who live in rural areas as well as those who live on the outskirts of urban areas.
Distance can be an even greater challenge if the person or family does not have reliable transportation. This is especially true in rural areas where public transportation does not extend to. Even with public transportation being available, the bus routes in most cities run on scheduled times and have limited hours of service. This means that anyone that works odd hours may not have access to the public transportation system. Furthermore, people that live farther away from grocery stores and that don’t have reliable transportation may have to be able to walk home, meaning that they can only purchase the amount of food they can carry in their hands. This also means that they have to make frequent trips to the grocery store to be able to have their nutritional needs met.
Similarly, individual abilities, such as family income, can greatly impact the food choices a person has access to. Purchasing healthy food is expensive, and if you want something that is free of pesticides or harmful chemicals (organic produce), it’s going to cost you even more money, money that you may not have. Additionally, eating healthy is not always a choice that people with low income have; the choices they are usually presented with are eating something (even if it is unhealthy) or starving for the next few days. You still have to have the energy to go to work and make money to pay your other bills. Roughly half of the American population made less than $35,000 annually, according to the Social Security Administration’s wage reports from 2019. These statistics have only increased as a consequence of the ongoing pandemic.
The neighborhood that a person lives in has a direct impact on their access to fresh food as well. Due to racist policies such as gerrymandering and gentrification, neighborhoods are separated based on the average income of their residents, and this usually means that the poor, (which are made up disproportionately of Black and Brown people), are pushed into underdeveloped areas and away from the up-and-coming neighborhoods in the urban centers. As a result, businesses are more reluctant to open up in impoverished areas, fearing that they won’t make much profit, and this extends to stores that sell fresh produce.
Food Insecurity: Some Hard Facts
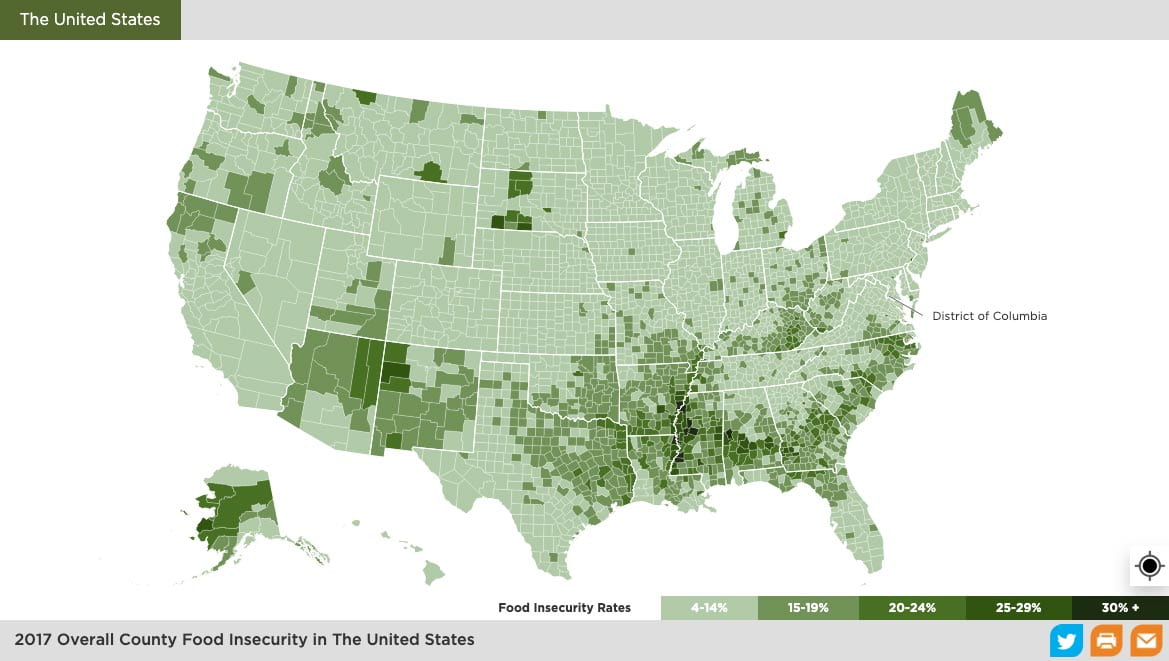
If the USDA definition of food deserts is applied in the United States, at least 19 million people live in food deserts. Looking closer to home, in Alabama, as of 2017, over 16% of its residents are facing food insecurities. Even right here in our own backyard, Birmingham Times reported in 2019 that around 69% of Birmingham residents live in food deserts. That is over half of the Birmingham population! As I have learned as recently as this semester during a Social Justice Café event, (a weekly event sponsored by the Institute of Human Rights at UAB that focuses on social justice issues), around 25% of UAB students are cutting meals, close to half of our UAB student population can’t afford to eat healthily, and over 35% of UAB students experience chronic food insecurity! I am one of these students; I am not ashamed to admit it. Despite how much I conserve and try to budget, I still cut meals constantly, I continue to not be able to afford to eat healthily, and I have been experiencing chronic food insecurity since before the pandemic. The reasons behind my struggles are no fault of my own; they are a domino effect of the various systemic failures that continue to plunge millions of hard-working Americans into poverty and as a result, food insecurity.
Eating Healthy: Why it’s a problem especially if you are poor

If a person has access to $20 for a week’s worth of groceries, spending it all on a couple of fruits and vegetables will not ensure that they can feed themselves and their loved ones for the next few days. What will help them make it through the week are spending on canned goods and processed food items that have a longer shelf life and cut down the time of food preparation. This means buying dollar menu items at fast-food restaurants or shopping at dollar stores for cheap snacks and pre-cooked meals. Low-income families who have experienced food insecurity for generations may not have acquired the knowledge to cook healthy food in a timely manner. They may not have had the resources to learn how to cook, or never had anyone to learn from.
Additionally, eating healthy requires that people cook with fresh, raw ingredients to avoid the preservatives and chemicals used in processed foods for a longer shelf-life. This also means cooking with items that may go to waste if not cooked in a timely manner. Most Americans struggling with food insecurity work low-income jobs, sometimes multiple jobs at a time, and the last thing they want to do is go home after a hard day of work and prepare meals for their family. Fast food is an easy, convenient alternative, and it is this convenience that has made them successful despite the unhealthy, low-nutritious food they sell.
Furthermore, this consumption of unhealthy foods with little nutritional value leads to chronic health issues, such as diabetes and heart disease. Even eating fruits and vegetables that have been grown with the use of pesticides and herbicides has been proven to expose those consuming them to toxic chemicals known to cause cancer. Therefore, to truly enjoy healthy produce, people have to purchase organic foods, which doubles the costs of groceries. Additionally, having adequate access to healthcare is another major challenge for those that live below the poverty line, and generally targets households that are already marginalized. These disparities have only been exacerbated due to the pandemic. As a consequence of the way that American healthcare is set up, most people living in poverty tend to avoid going to the doctor unless they absolutely have to, which further perpetuates the cycle of reactionary medical care rather than a precautionary one. Food insecurity is also surrounded by stigmatization, blaming the starving people for failing to put food on the table for themselves and their families instead of focusing on why this trend is common amongst almost half of the country’s hard-working citizens.
Non-Government Food Aid and Government Food Aid

Well, what about the government? Doesn’t it help those that are facing food insecurities? Government food aid comes in the form of SNAP/EBT benefits, commonly known as “food stamps,” and while it has helped many people struggling with food insecurity, this program has a lot of issues with it (too many to discuss in this blog). For today, however, let’s just examine some of the eligibility requirements to even qualify for food assistance. For one, Congress sets a threshold, requiring that people applying for the program must prove to the government that their income and expenses together show that they are living over 100% below the poverty line.
Furthermore, states can also add additional requirements such as passing a drug test or passing a background check. Some states disqualify applicants that have a criminal history from receiving assistance. If you’ve read my previous blogs about the realities of re-entering society after being imprisoned, you know why this is problematic.
Additionally, if the applicant is an immigrant, legal or illegal, qualifying for food assistance is almost impossible. Those who think that citizenship should be a requirement for food assistance don’t understand what human rights are. Food is a necessary resource that ALL humans have to have, and any person struggling to eat deserves to be helped, regardless of their citizenship status. There is also a requirement that people applying for assistance should have a job working at least 20 hours a week. This means that if you are unemployed, you cannot qualify for food assistance. That is exactly when you need the most help when you have no income or are transitioning from one job to another. On top of all these extensive eligibility requirements, if you are on strike, expressing your right to protest, something secured to you by the Constitution of the United States of America, you will not be able to qualify for food assistance. These conditions that require the people struggling with poverty to prove they are poor enough to receive assistance are demeaning, insulting, and undignifying to those who require the aid.
There are local non-profit groups and state institutions that provide food banks and food pantries where people can go to access food, but these places are usually located in more populated areas, meaning that people who live in rural areas or on the outskirts of cities face additional struggles accessing these food aid institutions. Transportation again becomes an issue for people living far from food banks and further limits their accessibility. Additionally, due to the stigma that surrounds food insecurity, people are made to feel guilty about their situation, and as a result, many avoid going to the food banks altogether.
How COVID has Made Food Insecurity Worse
The recent pandemic has changed many aspects of day-to-day life for people around the world. It has intensified the struggles of many Americans who were barely making it through life before the virus took hold. This same trend holds true when analyzing the pandemic’s impact on people experiencing food insecurity in America. The number of people struggling to feed themselves and their families has increased from 19 million in 2017 to over 50 million people in 2020. This is understandable, as many Americans lost their jobs during the shutdown of the economy, and many did not qualify for unemployment benefits.
Furthermore, due to the unhealthy nature of cheap foods, many Americans are experiencing malnutrition, dealing with obesity, diabetes, and heart problems, among other health issues. These health conditions have made them more vulnerable to catching the virus, and without an income, paying for healthcare becomes a major issue. Additionally, health insurance in America is tied to employment, and many Americans lost their jobs due to the economic shutdown, and as a result, also lost their health insurance coverage. All these factors have collectively worsened the lives of the poor and marginalized communities, adding to the growing financial instability and food insecurities these families face.
What Can We Do About It?

There are a lot of systemic issues to unpack that either leads to or exacerbates food insecurities. These issues need to be addressed through public policies that would help those struggling to eat by putting more money back into their pockets. These measures include pressuring our local policymakers to support legislation that would increase wages, lower eligibility requirements to access federal food aid, make healthy food more affordable and accessible, provide better public transportation, make healthcare affordable and accessible, and regulate businesses that exploit people to meet profit margins. All these things could help destigmatize food insecurity in our society and empower people to help themselves.
While food insecurity is a systemic issue that needs greater attention from our policymakers, there are still things that we can do ourselves. First, for those who are experiencing food insecurity here on campus, a resource called Blazer Kitchen is available for students and staff members, and their families to take advantage of. Blazer Kitchen is an onsite food pantry for those experiencing food insecurity. I’ve used Blazer Kitchen before, and while it is still a newly growing program, I have been grateful to have this resource at hand.
Second, for those who want to help reduce food waste, those who wish to shop at home, or those that have transportation limitations, Imperfect Foods is an online delivery service that has partnered with Feeding America (an organization aimed at ending food insecurity) to find a sustainable way to cut down food waste while simultaneously providing access to healthy foods for people who are food insecure. So much food gets wasted due to issues of over-harvested crops, changes in packaging, or even due to cosmetic imperfections that don’t always pass the scrutiny of the retail buyers. Instead of letting all this food go to waste, imperfect foods, and other such companies, strive to make use of these goods. This service also addresses the issue of transportation by having these imperfect goods delivered to your house.
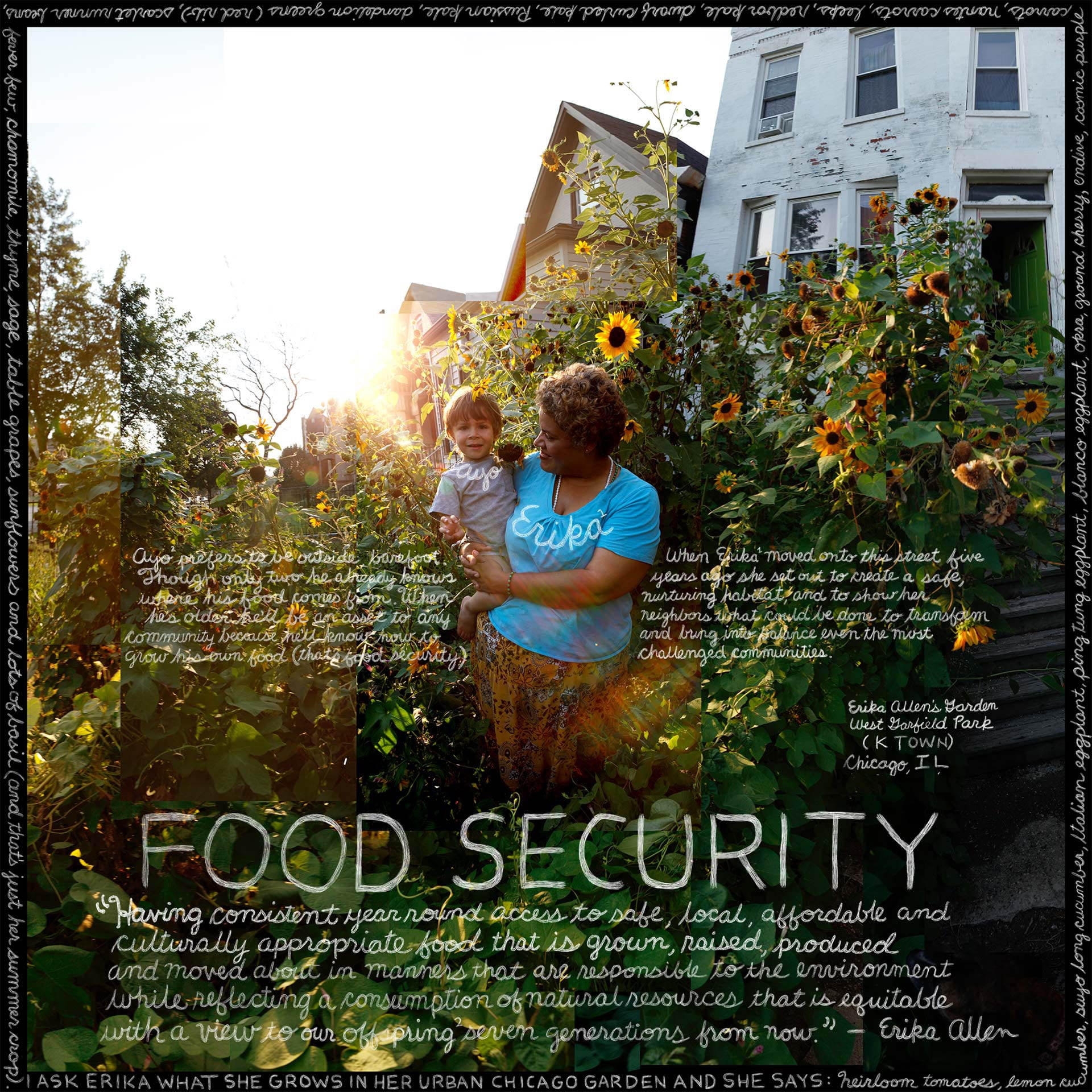
Finally, only people who live on properties with land can have access to personal produce gardens right now. Sponsoring local community gardens around the country can help educate people on how to grow their own food, can provide jobs for people to maintain these gardens, and provide access to healthy food options within walking distance. Localized community gardens can also decrease the carbon footprint left behind by massive corporate grocery stores that have to transport goods across states and can cut down on food waste as well. Also, share your experiences with food insecurity; let others know that you are experiencing it too. This helps start the process of destigmatizing this issue while educating others about the realities and complexities tied into your experiences. If you have the means to, donate to food banks and other such nonprofit organizations that provide help for those who desperately need it. Even if you never get to meet the people you are helping, know that they still greatly appreciate it. I know I do.