The coronavirus has spread to virtually every country of the world, but due to differences in privilege and access to resources, many countries are unable to adequately address this pandemic as well as other countries are. However, for countries in the Middle East, in addition to these differentials, the pandemic has also further exacerbated many preexisting problems that the region faces, namely political, economic, and social unrest. While this outbreak has had ramifications on several facets of life in the Middle East, this blog post will be focusing on the outbreak’s impact on sectarianism and the refugee crisis.
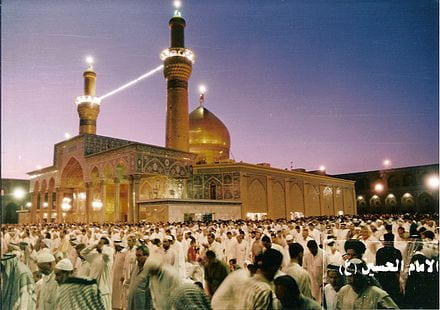
The Middle East is marred by the Sunni-Shia conflict, and geopolitics are heavily influenced by this divide. Because of this, the divide is often invoked when something disastrous occurs in the region, with each side blaming the other, and the coronavirus outbreak has proven to be no exception. Although the coronavirus has spread to all Middle Eastern countries, Iran, a Shia-majority country, has been disproportionately impacted; as of March 31st, Iran has had 44,605 coronavirus cases and 2,898 deaths, making it one of the countries with the most cases in the world. Further, Iran has now been identified as the source of spread to other Middle Eastern countries; some of the earliest identified cases in the Middle East were all of people who had recently traveled to Qom, one of the holiest cities in Iran. Despite the fact that people were aware of the outbreak in Iran, visitations to holy shrines in Iran were not discouraged, and people continued to travel to these holy sites. Any large gatherings during this time pose a risk, but shrine visitations are especially risky; many people engage in practices at shrines, such as kissing and touching the shrines, that lead to an increased likelihood of spreading. Since the outbreak is speculated to have spread from Qom, the city where one of the holiest shrines, the shrine of Sayyida Fatima al-Zahraa, is located, it is not unlikely that transmission did occur like this.
Because the spread has been identified as coming from Iran, many Sunni-majority countries in the Middle East have used this as an opportunity to justify further prejudice and discrimination against Shia Muslims. For example, Shia Muslims in Saudi Arabia who recently traveled to Iran for shrine visitations were labeled as traitors, leading some to call for their execution. In other countries, such as Lebanon, preexisting sectarian conflict has only gotten worse. It has been claimed that the first case in Lebanon came from Iran, leading many to blame the Shia Muslim population of Lebanon. Further, the Lebanese government continued to allow flights from Iran up until mid-March. Due to this, many have criticized Iran’s influence in Lebanon, specifically its influence on the government.
A Syrian refugee camp. Source: Yahoo Images, Creative Commons.
Despite the scarcity of resources and bleak outlook for refugee camps, measures have been taken to ensure that refugees are protected as best as they can be from the coronavirus. For example, many refugee camps have been sanitized with anti-bacterial spray. Certain organizations, such as Islamic Relief, have donated supplies, including rubbing alcohol and medicine that treats certain symptoms of the coronavirus, to ensure that if an outbreak does occur within a camp, there are some necessary resources available. Finally, the UNHCR has appealed governments for $33 million in funds to provide refugees access to hygiene kits, protective gear, and sanitary water, among other things, that could help deter the spread of the coronavirus.
Recently, an IHR Intern wrote a blog about racism and discrimination that arises during outbreaks such as this one. While Asians have largely been victims to racism during this period, in the Middle East, Iran and Shia Muslims have been targeted, highlighting that people do indeed try to blame such events on others when, in reality, there is no one that should be blamed. Further, times like this also highlight the level of privilege many of us live in; while we have the privilege to access resources and to distance ourselves from one another, other groups who lack such privileges, namely refugees, cannot practice any of these things. Thus, while we are all impacted by this outbreak, it is important to recognize that many people, in addition to worrying about the coronavirus, face other obstacles during this time as well, and these groups should be kept in mind.
How long ago this seems now, in the midst of the COVID-19 crisis. The impetus of this blog post is Nelson and Maggie’s desperate appeal to help support their people who have been hit extremely hard by this crisis, and to show how COVID-19 affects people in the developing world.
COVID-19 in developing countries
While we have raised awareness of what this crisis means for some of the most vulnerable and marginalized in our own society, having to deal with a pandemic in developing countries is a whole different endeavor. The virus itself and the sickness it causes are only half of the danger. Major societal issues such as widespread poverty, economic deprivation, and lack of access to water, food, sanitation, and healthcare present huge challenges for people in the Global South. The COVID-19 crisis threatens already fragile economies and has the potential to negatively impact human rights, education, basic resource allocation, and food security. Under-resourced healthcare systems and hospitals are likely to be overwhelmed, creating a probability for higher death rates. A majority of people in developing countries also lack access to water and soap, increasing the likelihood of infections and facilitating the spread of the disease. In addition, there are no social safety nets or government bailouts for workers and businesses, exacerbating scarcity, political struggles, violence, and poverty.
Women and children in a Maasai house at Nashulai Conservancy. Source: Nora Nord, nashulai.com
In other words, it is not just the virus that threatens people’s lives in developing countries, but the whole context – poverty, underdevelopment, structural violence, lack of government resources to respond to the pandemic – that puts lives in peril and threatens the existence and survival of whole communities. People in developing countries are doubly at risk. This crisis will leave deep scars, not only with regards to lives lost, but also with regards to international development gains made in the last decades in development, human rights, and human dignity. These are the issues Nelson and Maggie are afraid of. They are not only worried about the immediate impact of this crisis on their people, but also about the setback this crisis will cause to the wildlife, economic, and cultural advances that have sustained and elevated their community for the last years and made Nashulai indispensable for their society. Their people, their project, and their way of life are in peril of survival.
What COVID-19 means for Nashulai Conservancy
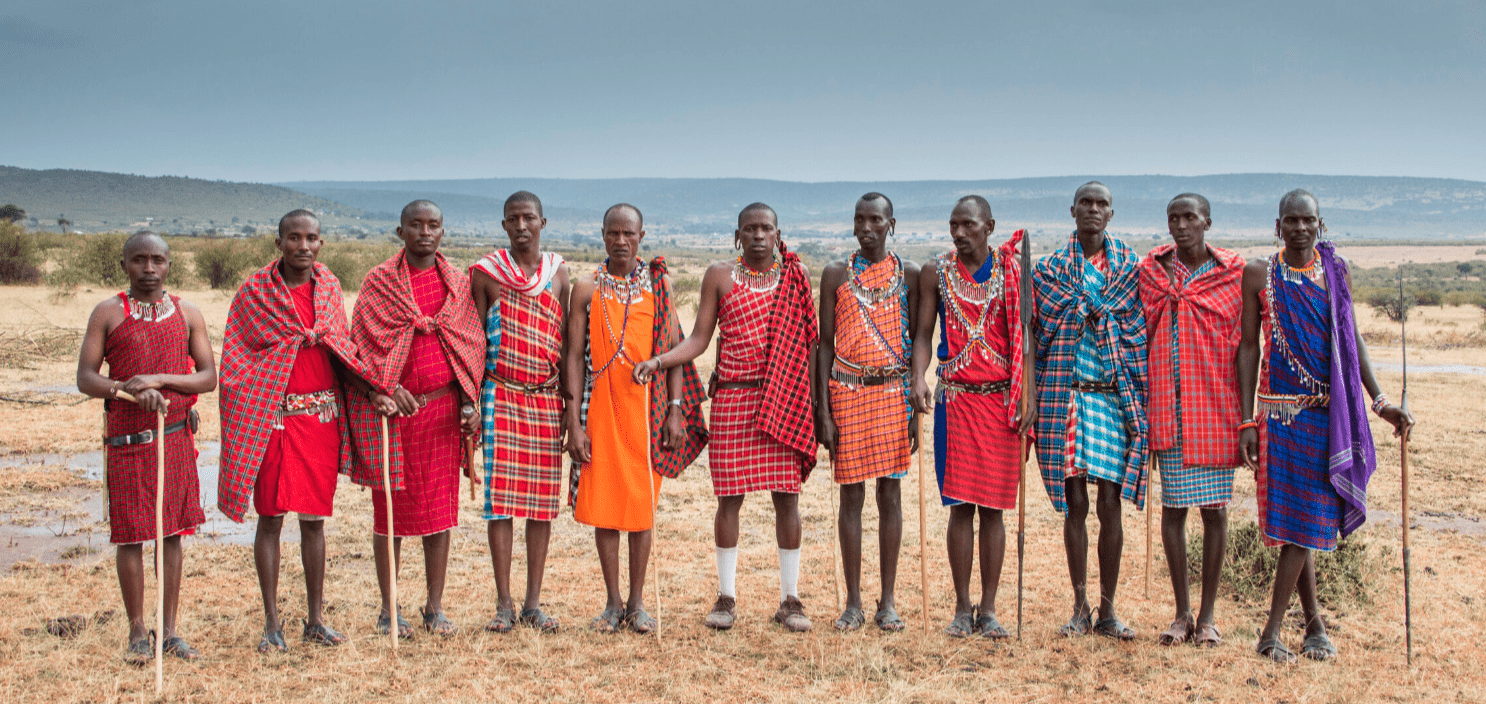
Nashulai is a community-led conservancy in the Maasai Mara in the southwestern part of Kenya, close to the border to Tanzania. The Maasai are an indigenous community of strong and brave warriors, but poverty and lack of development have negatively affected their quality of life. Most Maasai exist on less than $1 a day, depending mostly on their livestock for food and income. More recently, due to Nashulai’s efforts, the community has been able to garner revenue through tourism by offering safaris and running guest houses and camps. About 2,000 people live on Nashulai’s 6,000 acre conservancy, and an additional 3,000 people live in the surrounding communities. Most of them reside in traditional Maasai villages, in which small dwellings arranged in a large circle for community living. Women, men, and children live together in small spaces and share food, resources, and chores with one another. Men mostly look after cows, sheep, and goats or work in local tourist camps and lodges, while women prepare food, raise children, and make jewelry and art work to sell to tourists. Livestock is sold on twice-weekly open markets in exchange for grains, oil, salt, and other basic necessities.
The Maasai live in close-knit communities where women, men, and children of different families share all aspects of everyday life. Source: Marianne Nord, nashulai.com
COVID-19 has put all of this in danger. The markets are closed due to government safety measures, leaving people without food and without income. Tourist streams have run dry, which means no money and no jobs (90% of employed Maasai rely on the tourist industry). The communal way of Maasai life is in direct opposition to the guidelines of social distancing and self-isolation. There is no running water in Maasai homes, making constant handwashing not an option. Healthcare in the rural areas of Kenya is difficult access in the best case, and Sekenani health clinic in the conservancy is not equipped to deal with COVID-19 cases. It is unclear what should happen to people who become infected. There is a lack of information and education about the crisis, and an absence of guidance of what the WHO guidelines of handwashing, social distancing, and self-isolation and quarantine mean for people in places like Nashulai. There is no electricity beyond solar power, and while some people have phones or radios, spreading news and information is extremely difficult.
The situation is dire. People are starving.
Nelson and Maggie have developed an emergency plan to provide each household with basic food items, to repurpose part of Nashulai’s tourist camp to isolate sick people, and find ways to educate the community about safety measures and health. They have established a strategy on how they can become self-sustaining in terms of food production and continue their important conservancy work over the next months. However, because their stream of revenue has been cut, they rely on us, their friends, to support them, the Maasai people in their community, and the long-term survival of their project.
Recently, select states and hospitals have issued guidelines for health providers that would potentially deny people with disabilities treatment for COVID-19. Two entities, Alabama Department of Public Health (ADPH) and Washington State Department of Public Health (WSDPH), have recently come under scrutiny because of their efforts to fulfill such guidelines.
ADPH’s Emergency Operations Plan suggests that ventilator support would be denied to patients with “severe of profound mental retardation”, “moderate to severe dementia”, and “severe traumatic brain injury”. This controversial protocol has recently grabbed the attention of Alabama Disability Advocacy Program and The Arc thus leading to a complaint with U.S. Department of Health and Human Services Office for Civil Rights (OCR) regarding discrimination toward people with intellectual and cognitive disabilities.
OCR swiftly responded to these concerns, as well as those from Kansas and Tennessee, by stating that, even in the case of pandemics, hospitals and doctors cannot undermine the care of people with disabilities and older adults. OCR Director Roger Severino exclaimed, “We’re concerned that crisis standards of care may start relying on value judgments as to the relative worth of one human being versus another, based on the presence or absence of disability,” and “…that stereotypes about what life is like living with a disability can be improperly used to exclude people from needed care.”
Also, with New York currently having most of the U.S.’s confirmed COVID-19 cases, they may very well be the first state to face the imbalance of available ventilators and patient demand. Disability advocates have recently decried verbiage in New York’s Public Readiness and Emergency Preparedness (PREP) Act that could provide immunity from civil rights for some patients. Thus, U.S. state and federal powers are playing tug-of-war with the status of disability rights during the COVID-19 crisis.
Not Today COVID-19 Sign on Wooden Stool. Source: Pexels, Creative Commons.
However, these concerns are not limited to the U.S. In the developing world, many people with disabilities are segregated from their communities in overcrowded facilities, while thousands of others are shackled and incarcerated. This weak enforcement of disability rights positions people with disabilities, in countries such as Brazil, Croatia, Ghana, India, Indonesia, and Russia, at-risk of further inhumane treatment by receiving limited or no appropriate care related to COVID-19. As a result, Human Rights Watch urges state and local authorities to return these populations to their families and demand they provide needed support and services within their communities.
Nearly every country in the world has ratified the United Nations’ Convention on Rights of Persons with Disabilities (CRPD) which aims to fulfill the human rights and fundamental freedoms of people with disabilities. More specifically, Article 25 of CRPD suggests people with disabilities have the right to non-discriminatory health care and population-based public health programs. Thus, nearly every person with a disability around the globe is associated with a governmental power that claims to be dedicated to fulfilling the promise of CRPD. However, in the wake of COVID-19, will these words be put into action?
These unprecedented events are a turning point for how we view our bodies, health, and communities. This is also an opportunity to view the world through the perspective of those in your community such as people with disabilities who represent an array of impairments, challenges, and experiences. Despite boredom and apathy being at the forefront of many people’s isolation, images of life versus death surround others, and for a good reason. In these decisive weeks, and likely months, there has never been a greater time for people in the U.S. and abroad to acknowledge that disability rights are human rights.
Coronavirus Public Alert Oslo. Source: Annikdance, Creative Commons.
At this point, I’m sure almost everyone knows about COVID-19. With schools shutting down, conferences being cancelled, and travel being restricted, even those in uninfected areas are affected. However, while some of us are most worried about washing our hands and not touching our faces, some people have to worry about discrimination. Those of East Asian descent are being discriminated against all over the world, whether they’re from China or not, whether they’ve been in infected areas or not, whether they’re sick or not. COVID-19 is bringing out racism that has laid dormant, and, unfortunately, this isn’t the first time it has happened.
Historically speaking—especially before the scientific knowledge we have now—large outbreaks were blamed on minority groups. In 14th century Europe when the Black Death occurred, many looked for an answer, and when they couldn’t find an answer, they found a scapegoat: the Jews. They were seen as nonconformists by the Christian majority and were subsequently blamed for the outbreak that would be known as the Black Death. Many were tortured until they made false confessions and killed, and their persecution continued centuries later.
Since then, almost every major outbreak has illuminated underlying racism within the global community: when syphilis appeared in Renaissance Europe every country blamed another; Irish immigrants were blamed for the 1830 cholera outbreak; and Mexicans and others from Latin American countries were discriminated against during the Swine Flu epidemic in 2009.
Most recently, the Ebola outbreak of 2014 brought out racism towards those of African descent. College admission was denied to two Nigerian students to Navarro College, and a Guinean high school soccer player attending school in Nazareth, Pennsylvania was heckled by the opponent’s fans, who chanted “Ebola” at him. Americans hesitated to shake hands with people of African descent, whether they were American or not, and the US imposed a travel ban to and from West Africa.
What we are seeing now with COVID-19, is similar to what we saw during the 2003 SARS outbreak. While the Ebola outbreak illuminated prejudices towards African Americans, in 2003, those of East Asian descent, regardless of their nationality were discriminated against in certain areas. The three Chinatowns in Toronto, Canada were empty for weeks, East Asians were constantly asked if they were sick when no one else was, and they were avoided when they went out in public. In Canada, there is the stereotype of yellow peril that labels Asians as “unsanitary, lower-class, and alien.” This stereotype obviously found root in SARS and only exacerbated these prejudices.
Spiritual Xenophobia. Source: George Ian Bowles, Creative Commons
Unfortunately, it seems like we haven’t learned from these numerous outbreaks, and the racism and xenophobia along with COVID-19 is way more widespread and way more violent. A man attacked an unidentified woman was attacked on the subway in New York, and reports say that the confrontation was a result of the Asian woman wearing a mask. Like in 2003, the discrimination is not restricted to people of Chinese descent: a man singled out a Thai American lady on a bus in LA. He gestured at her while saying that “every disease ever came from China.” Finally, in Indiana, two men of Asian descent were denied a room at a hotel and told that if they were Chinese, they’d be “picked up and quarantined for two weeks.” All of these attacks were before any deaths occurred in the US.
These incidents aren’t unique to the Untied States either. In London, a student from Singapore was attacked in a busy shopping area. While he was being attacked his assailants told him, “I don’t want your coronavirus in my country.” He was left with fractures on his face, and he might need reconstructive surgery.
The racism that is emerging is not new, it has just been hidden. The fear that everyone is feeling is being redirected towards previous biases. The student from Singapore reported that he had been experiencing racist comments for the entire two years he had been studying in London. Because COVID-19 originated in China, the racism already present towards those of Asian descent has been exposed, and thanks to misinformation, it continues to grow. Fear has been shown to bring out the racism that already exists within people, not cause it.
In times like these it’s important to know the facts because that’s how we fight this discriminatory fear culture: Asians are no more likely to have COVID-19 than the rest of us. No one is any more likely to get COVID-19 because of their race or ethnicity. Despite the virus originating in China, there is no evidence Chinese people or Asians are predisposed to infection. Secondly, just because someone of Asian descent is wearing a mask, it does not mean they’re sick. In many East Asian cultures, it is normal to wear a mask year-round, not just when you’re sick.
It’s important to spread the facts. One of the biggest factors in discrimination is ignorance, so education is the best way to fight it. People are scared, and that is bringing out the prejudices they’ve kept hidden and might not even know they had. Additionally, catch and correct yourself when you think or do something with prejudice. Start improving our global community by improving your own thoughts.
COVID-19 is a pandemic, and it’s a serious infection, especially for the elderly and those with preexisting health conditions. However, the racism and xenophobia are spreading just as fast. As a global community, we shouldn’t add to the burden of this disease by using it as an excuse to be discriminatory.
As countries around the world continue to fight the outbreak of the coronavirus and deal with the disease is causes (COVID-19), the question arises how this public health crisis affects human rights. It is essential that we not ignore human rights during this crisis, even if our primary focus is fighting the outbreak and finding a cure for the disease. The epidemic and the response to it have a major effect on people’s lives, and thus are guided and impacted by human rights. Human rights cannot be an afterthought, but need to be worked into both public and private responses.
To follow up on my colleague Dr. Peter Verbeek’s earlier blog post, I will focus my considerations on two issues: 1) how public policies and legislation in response to the coronavirus and COVID-19 affect human rights; and 2) the broader human rights consequences of the proposed and implemented public health measures.
May public health policy limit human rights?
Most countries have statutes that allow for limitations to human rights in times of national emergencies or major public health threats. According to international law (and in most democratic states constitutional law), these limitations have to be necessary, proportionate, and related to clear and lawful public aims. They also have to be implemented in accordance with existing laws and the greatest measure of transparency.
In response to the coronavirus, emergency legislation in many countries (see for example in the U.S., U.K., Canada, or Australia) allows health departments and public health officials to impose a number of measures that affect people’s lives and their human rights. These measures include detaining people to be screened, collecting their health information, and putting them in isolation. People who do not comply with orders by public health officials or obstruct their work, refuse detention, leave a place of isolation, or supply misleading information can face criminal charges. For example, when a woman was evacuated from Wuhan and quarantined at Travis Air Force Base in California asked to leave the facility, California authorities issued an order forcing her to stay against her will.
While these types of measures might be necessary during such emergencies, it is worth noting that they do interfere with basic human rights, especially the right to liberty (UDHR Article 3), protection from arbitrary detention (UDHR Article 9), right to privacy (UDHR Article 12), and freedom of movement (UDHR Article 13). Considering the significance of these rights and freedoms and the grave consequences that can come from violating them, it is vital that government policies impede individual freedoms and human rights as little as possible. Further, any interference on human rights has to be based on strongest scientific evidence available (as opposed to, for example, racist or xenophobic justifications).
The ceiling of the UN Human Rights Council in Geneva. Source: United States Mission Geneva, Creative Commons
There are a number of important ways to achieve this.
To ensure the protection of privacy and other rights, only data directly relevant to combatting the coronavirus outbreak should be gathered from individuals. The Center for Disease Control (CDC) has wide-ranging powers in case of emergencies, including obtaining clinical specimens and data from persons affected by an outbreak, obtaining data from healthcare facilities, enforcing control measures including quarantine, and seizure or destruction of private property. While some of these measures might be needed to stop the spread of a virus, it is important that the principles of necessity and proportionality are at the front and center of response policies to guarantee the respect for human rights.
Public health organizations, as well as the government, need to establish official communication channels that remain open for detained and quarantined people. Moreover, those subjected to restrictions such as detention and quarantine should have the ability to appeal their situation and voice their concerns regarding their treatment.
Officials, as well as the public, have to recognize that those in quarantine or detention are in an extremely difficult situation. In addition to their medical state, they are often socially and economically vulnerable. The stigma that often accompanies quarantine and/or detention can lead to exclusion, emotional difficulties, and mental health issues. Similarly, loss of income or jobs can lead to short-term and long-term problems for affected people. For their part, governments should act to mitigate the negative consequences of public health policies and be aware of underlying socioeconomic conditions, potential human rights violations, and structural violence.
The duration and severity of necessary limitations on human rights should be clearly communicated. It is not just the extent of human rights limitations that matter, but also how long they are set in place. The so-called “war on terror”, for example, was originally launched as a response to the terror attacks of 9/11, but it has persisted for decades, with legal authorities extending well beyond their original goals.
The human rights consequences of fighting the coronavirus
This brings me to the second part of my post, which focuses on the broader human rights and societal consequences of the current coronavirus outbreak. As Mary Bassett and Natalia Linos of Harvard’s FXB Center for Health and Human Rights write in the Washington Post, “[e]pidemics emerge along the fissures of our society, reflecting not only the biology of the infectious agent, but patterns of marginalization, exclusion and discrimination.” Beyond the more immediately obvious issues of how quickly the virus spreads, how many people will die, and how our healthcare system is affected, we need to ask ourselves about the societal effects of public health threats.
The most significant question is: who is the public? Who are public health responses designed for? Race, gender, caste, class, migration status, disability, ethnicity, religion, sexual orientation and gender identity, living conditions (urban v. rural), and other attributes determine the level of inclusion or exclusion of a person or group in society and their vulnerability in case of crisis. Even when measures seem neutral on the surface, public health responses to infectious diseases tend to follow a “utilitarian logic”, which can lead to unintended consequences and discrimination. For example, results are often gendered: Women tend to be caretakers of children and older people, making them the first to have to skip work when children are out of school or elderly parents fall ill. They are also often front-line healthcare providers, and any family-related responsibilities for these women can lead to shortages of available health personnel. Other advice, such as “social distancing”, cannot be upheld in prisons, public transportation, or migrant camps, and are therefore only useful for the privileged who live in their own flats or houses and can use their cars for transportation. In some cases, public health responses emphasize xenophobic or racist tendencies and reinforce societal divisions. There are already a number of stories and occurrences people of Asian descent shared about sneezing or coughing in public and experiencing responses ranging from angry looks to outright racist comments. Also, not all people have access to information if it is not prepared in minority languages, accessible formats, and spread through different means (e.g., illiterate people will need audio or visual announcements).
This situation is particularly problematic in the U.S. healthcare system, as it excludes people based on employment and/or immigration status and on the availability of financial resources. The large number of people without access to health insurance will not have the same level of information, testing, or treatment available to them as those with health insurance, and they face additional worries about financial burdens associated with seeking care. Further, private companies can decide how much to charge for treatments of the virus or vaccines without concern about affordability.
In my mind, a purely market-based allocation of healthcare resources in times of COVID-19 is not only unethical, but a human rights violation. Article 25 UDHR calls for everyone to have “the right to a standard of living adequate for the health and well-being of himself and of his family, including food, clothing, housing and medical care and necessary social services, and the right to security in the event of unemployment, sickness, disability, widowhood, old age or other lack of livelihood in circumstances beyond his control.” How far we are from this ideal! Viruses and pandemics don’t care about a person’s legal, economic, or social status, but because of lack of human rights-based public health responses, crises will have differing impact on rich, privileged people as opposed to poor, disenfranchised populations. As UN High Commissioner for Human Rights Michelle Bachelet stated, “people who are already barely surviving economically may all too easily be pushed over the edge by measures being adopted to contain the virus.” The search for an inclusive public health response and a more equitable and accessible healthcare system is even more urgent and important in times of the coronavirus and COVID-19.
Distorted world? Source: Kevin Dooley, Creative Commons
Where does this leave us?
What happens next and the way our political leaders handle this crisis is therefore crucial. If authorities take a heavy hand, twist the truth, and/or compromise hard fought for fundamental freedoms and human rights, the public might be less willing to cooperate in a future crisis situation. Successful interventions in public health crises do not only depend on the level of control issued and the sophistication of medical responses, but also, and most importantly, on whether or not the people trust the government to handle the crisis, to communicate transparently, and to be accountable to its citizens. It also depends on solidarity and community building – whether people cover their coughs and sneezes, self-isolate when they think they got infected, and not hoard scarce supplies to the detriment of others. Public participation and agency of all people is therefore a key component of managing the disease successfully.
As the UN High Commissioner for Human Rights and my colleague Peter Verbeek pointed out, it is vital to structure any response to the coronavirus outbreak holistically, and that includes respect for and protection of human rights. It means to develop a transparent public response based on principles of equity and accountability for all actors involved, including the private sector. It also requires taking care of those most vulnerable in a crisis and protecting the most marginalized in a society, both medically and economically. Human rights cannot be an afterthought in epidemics. How governments handle the coronavirus and their response to COVID-19 might as well set a precedent for human rights in the future. Let’s hope that this crisis will be an opportunity to see the value of human rights, public participation/democracy, and multilateralism.
by Peter Verbeek, Ph.D. (Associate Professor, Program Director MA Anthropology of Peace and Human Rights)
Source: Yahoo Images
On March 6, 2020, the UN High Commissioner for Human Rights, Michelle Bachelet, issued a statement calling for an holistic human rights based approach to combat COVID-19. She wrote, “As a medical doctor, I understand the need for a range of steps to combat COVID-19, and as a former head of government, I understand the often difficult balancing act when hard decisions need to be taken.” However our efforts to combat this virus won’t work unless we approach it holistically, which means taking great care to protect the most vulnerable and neglected people in society, both medically and economically.” She added, “COVID-19 is a test for our societies, and we are all learning and adapting as we respond to the virus. Human dignity and rights need to be front and centre in that effort, not an afterthought.”
To heed Dr. Bachelet’s call we must remind ourselves of the fact that human rights are universal and inalienable, indivisible, interdependent and interrelated. We also must recognize that the essence of human rights is human dignity. All human rights arise from it and all human beings are born with it and posses it throughout their life span. Human dignity is not measured on a sliding scale. To illustrate, there is no difference in human dignity between that of the office holder of the Presidency of the United States and the migrant at the US Southern border. The accused in the court proceeding has the same human dignity as the judge presiding over her case. The convict and the prison guard do not differ in their human dignity. The human dignity of the disabled veteran is the same as that of the person pushing her wheelchair. And the human dignity of the COVID-19 patient in the isolation ward is the same as that of the health-care worker taking care of him.
The recognition of our shared human dignity and the safeguarding of the rights that arise from it is a powerful unifier in troubled times. Now that we are faced with a near global outbreak of an until recently unidentified corona virus we can stand united in the recognition that every person on this Earth has an irrevocable right to health care and security in the case of illness (UDHR, Article 25). With rights come responsibilities, and the unifying power of universal human rights is the way that each of us in accordance with our specific context and abilities has a role to play in safeguarding access to appropriate preventive and interventional health care and personal security regarding COVID-19. Our individual roles are necessarily varied, from driving a neighbor without proper means of transportation to a health care facility, to following “doctor’s orders” concerning personal hygiene or social distancing. If infected or taken ill we have a right to receive the best available care and the responsibility to follow the guidelines in place so as to minimize the risk of infecting others. Each of us has a responsibility to listen to the relevant and evolving science as communicated by medical experts, and each of us has the responsibility to comply with the local and national guidelines that are based on this science.
Some of those taken ill with COVID-19 will die in spite of our best efforts to care for them and protect them. If the fight to save their life is at the cusp of being lost we have the responsibility to see to it that their death reflects the human dignity that they possess. Medical science does not yet have the answer to the question of how to protect oneself conclusively against viral infections such as the current corona virus. That realization, while sobering, should not keep us from doing all we can in terms of what we do know about prevention. There is much that we can do to limit the risk of infection, provided we follow the relevant science. The human rights motto is that any infection, or worse, any death, linked to insufficient preventive measures is one too many, and we all stand united in this through the human dignity that each of us possesses.
UAB is an Equal Opportunity/Affirmative Action Employer committed to fostering a diverse, equitable and family-friendly environment in which all faculty and staff can excel and achieve work/life balance irrespective of race, national origin, age, genetic or family medical history, gender, faith, gender identity and expression as well as sexual orientation. UAB also encourages applications from individuals with disabilities and veterans.